

Short Dive: The Sunscreen Guide Nobody Gave You (Part 1)
A third of Gen Z failed a basic sun safety quiz. Here's the research-backed guide that actually explains why this matters and what to do about it.

A 2026 survey asked Gen Z basic questions about sun safety. A third of them failed. Not struggled - failed. D or F territory.
That’s not a knock on anyone’s intelligence. It’s a knock on where the information has been coming from. The same survey found that 36% of Gen Z say influencers are their primary source of skincare information and a lot of what’s circulating is confidently wrong. A tan being a sign of “healthy” skin. SPF only mattering on sunny days. A higher SPF number meaning you can apply less. These aren’t fringe beliefs. They’re common enough to show up in a national survey.
Meanwhile, “skin longevity” has become the defining skincare conversation of 2026, the shift from fixing damage after it happens to keeping skin functioning well for decades. Which makes this the perfect, slightly ironic moment to point out: the single most powerful skin longevity tool already exists, it’s been sitting in your bathroom cabinet the whole time, and most people are using it wrong or not using it enough.
This short dive is the sunscreen guide that should have existed years ago. What UV radiation is actually doing to your skin at a cellular level. Which myths are costing you the most. The honest, current state of the mineral-versus-chemical debate, including a few 2026 developments that haven’t filtered into mainstream skincare content yet. And in Part 2, the practical guide: how much to actually use, the vitamin D balance, and what to do if your skin is acne-prone, sensitive, or prone to pigmentation.
Let’s start with the biology.
Chapter 1: What UV Radiation Actually Does to Your Skin
Two Types of Rays, Two Different Kinds of Damage
Sunlight that reaches your skin contains two types of ultraviolet radiation that matter for skin health: UVA and UVB. They’re often talked about as if they’re interchangeable. They’re not. They damage skin through different mechanisms, at different depths, with different consequences and understanding the difference is the foundation for understanding why SPF alone isn’t the whole story.
UVB is the shorter-wavelength ray. It mostly affects the outer layer of your skin (the epidermis). This is the ray responsible for sunburn, and it works by directly damaging your skin cells’ DNA. When UVB hits a skin cell, it causes specific kinds of DNA damage where the building blocks of your DNA fuse together incorrectly. Your body has repair systems for this kind of damage, but they’re not perfect and the damage that doesn’t get repaired correctly is the kind that’s strongly linked to skin cancer development over time.
UVA is the longer-wavelength ray, and it penetrates much deeper, all the way into the dermis, the layer of skin where collagen and elastin live. This is the layer responsible for your skin’s structure, firmness, and bounce. UVA’s main damage pathway isn’t direct DNA breakage. It’s oxidative stress: UVA exposure generates reactive oxygen species inside skin cells, which then activate enzymes called MMPs (matrix metalloproteinases) that actively break down collagen. Research comparing UVA and UVB damage at the cellular level found that UVA specifically promotes the breakdown of dermal collagen fibres and triggers inflammation, while UVB primarily affects the surface cells. UVA penetrates roughly 1.6 times deeper into skin than UVB, which is exactly why it’s the ray most responsible for wrinkles, sagging, and loss of elasticity, while UVB is more associated with burning and surface damage.
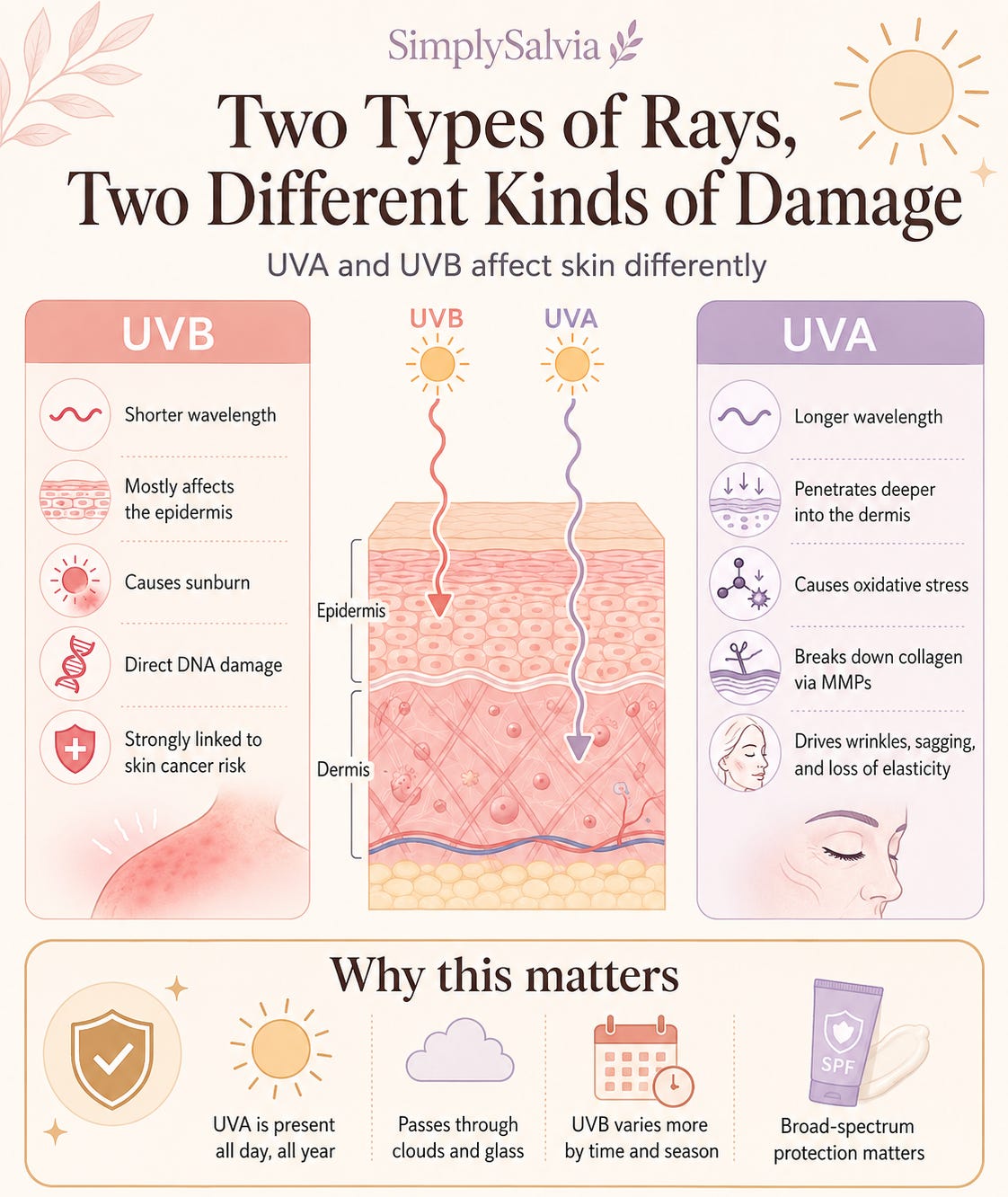
Here’s the part that matters most: UVA is present at consistent intensity all day, every day, all year round, including through clouds and through glass windows. UVB intensity varies much more by time of day and season. This is why “I’m not getting sun damage, it’s cloudy” or “I’m inside all day” are two of the most common and most costly misunderstandings about sun protection. The ray responsible for collagen breakdown doesn’t care whether you can feel the heat.
Why the Damage Is Invisible Until It Isn’t
This is the part of “skin longevity” content that often gets skipped: by the time photoageing is visible; fine lines, uneven texture, brown spots, looser skin, the damage has usually been accumulating for years, sometimes decades.
The collagen breakdown triggered by UVA exposure happens immediately at a cellular level, every time skin is exposed without protection. But collagen is abundant, and the visible effects of its breakdown only become apparent once a critical threshold has been crossed. Research using collagen gels found that UVA radiation specifically causes hardening and loss of elasticity in collagen, more so than UVB and that this effect compounds with cumulative exposure over time. This is why someone who’s 24 and never worn SPF consistently doesn’t look damaged yet, but the cellular process that produces visible photoageing at 35 or 40 has already been running for years.
This delay between cause and visible effect is precisely why prevention has to start before there’s anything to see. It’s the same logic that applies to bone density, as covered in a previous Between Saturdays; peak collagen density and skin structural integrity are being built and maintained right now, in your teens, 20s, and early 30s, whether or not you’re paying attention to it.
The DNA Damage Layer: Why This Isn’t Just About Wrinkles
It’s worth being direct about the more serious side of this conversation, because most skincare content focused on “skin longevity” and ageing tends to underplay it.
UVB radiation directly forms specific DNA lesions; cyclobutane pyrimidine dimers and related photoproducts, that are strongly associated with skin cancer development when they aren’t correctly repaired. UVA contributes too, primarily through oxidative DNA damage, and has its own documented association with melanoma risk. The cumulative, unprotected exposure that produces visible photoageing over years is the same cumulative exposure that raises skin cancer risk over the same period.
Even mild psychological stress appears to amplify UV damage at the cellular level. A 2024 study found that stress occurring during UVB exposure degraded collagen function by suppressing its production, compounding the damage already happening from the UV exposure itself. This is a genuinely interesting finding: the stress-skin connection covered in earlier Simply Salvia content isn’t separate from sun damage, it appears to interact with it directly.
None of this is meant to be alarming for its own sake. It’s meant to explain why “I’ll start caring about sunscreen when I’m older” is backwards. The damage that shows up later is being determined now.
Chapter 2: The Myths Costing You the Most
This is the chapter built directly around the specific gaps the 2026 AAD survey identified, the beliefs that are common, confidently held, and wrong.
“A Tan Means Healthy Skin”
This is the single most damaging misconception in the survey results, and it’s worth being completely clear about: there is no such thing as a healthy tan. Any visible tan is a sign of UV damage that has already occurred, it’s your skin’s melanin-producing cells responding to DNA damage by producing more pigment as a protective (and imperfect) response. A tan is your skin’s distress signal, not a sign of vitality.
This doesn’t mean sunlight itself is the enemy, sensible sun exposure has real benefits, covered in Chapter 5 of Part 2. It means that the specific outcome of “getting a tan” visible skin darkening from UV exposure is, by definition, evidence of damage having occurred, not a wellness goal to pursue.
“SPF Is Only Necessary on Sunny Days”
UV radiation, particularly UVA, isn’t meaningfully reduced by cloud cover. Up to 80% of UV rays can penetrate cloud cover, meaning a grey, overcast day can deliver nearly as much UVA exposure as a clear one. This is one of the more counterintuitive facts in sun safety, because cloud cover reduces the heat you feel, which intuitively (and wrongly) reads as reduced UV exposure.
The practical implication: daily SPF isn’t a summer habit or a beach-day habit. It’s a daily habit, regardless of forecast, because the ray most responsible for long-term collagen damage doesn’t fluctuate with visible weather conditions.
“Higher SPF Means I Can Apply Less”
This is backwards, and it’s a genuinely costly misunderstanding. SPF protection doesn’t scale linearly with the number, it scales logarithmically, and crucially, the SPF rating on any bottle is only achieved at a specific application amount (2mg per cm² of skin, which works out to roughly a nickel-sized amount for the face). Most people apply somewhere between a quarter and half of this amount in real-world use, which means an SPF 50 product applied at half the recommended amount delivers closer to SPF 10–15, not SPF 25.
A higher SPF number gives you more margin for under-application, not permission to under-apply. The number on the bottle is a ceiling you only reach with the correct amount.

“My Foundation/Moisturiser Has SPF, So I’m Covered”
Multi-purpose products with SPF built in are genuinely useful as a layer of protection, but they’re rarely sufficient as the only layer, for two reasons. First, people apply far less foundation or tinted moisturiser to their face than the amount needed to achieve the labelled SPF, typically a fraction of a nickel-sized amount, when full SPF protection requires significantly more. Second, many of these products aren’t reapplied through the day the way a dedicated sunscreen would be, even though SPF protection degrades with time and UV exposure regardless of the product format.
The practical guidance dermatologists give consistently: treat SPF-containing makeup as a bonus layer on top of a dedicated sunscreen applied properly underneath, not as a replacement for one.
“Sunscreen Causes More Harm Than the Sun Itself”
This belief has gained traction from genuine, evolving research on chemical sunscreen absorption, covered honestly in Chapter 3 but it’s frequently overstated into “sunscreen is dangerous,” which isn’t what the evidence supports. The honest research distinguishes between specific chemical filters with documented absorption and hormonal interaction concerns, and the category of sunscreen as a whole, which has decades of evidence supporting its role in reducing photoageing and skin cancer risk. The next chapter goes into this distinction properly.
Chapter 3: Mineral vs. Chemical Filters. What the Evidence Actually Says in 2026
This is the part of the sunscreen conversation that’s evolved the most recently, and it deserves a more current and more nuanced treatment than most existing content gives it.
How Each Type Works
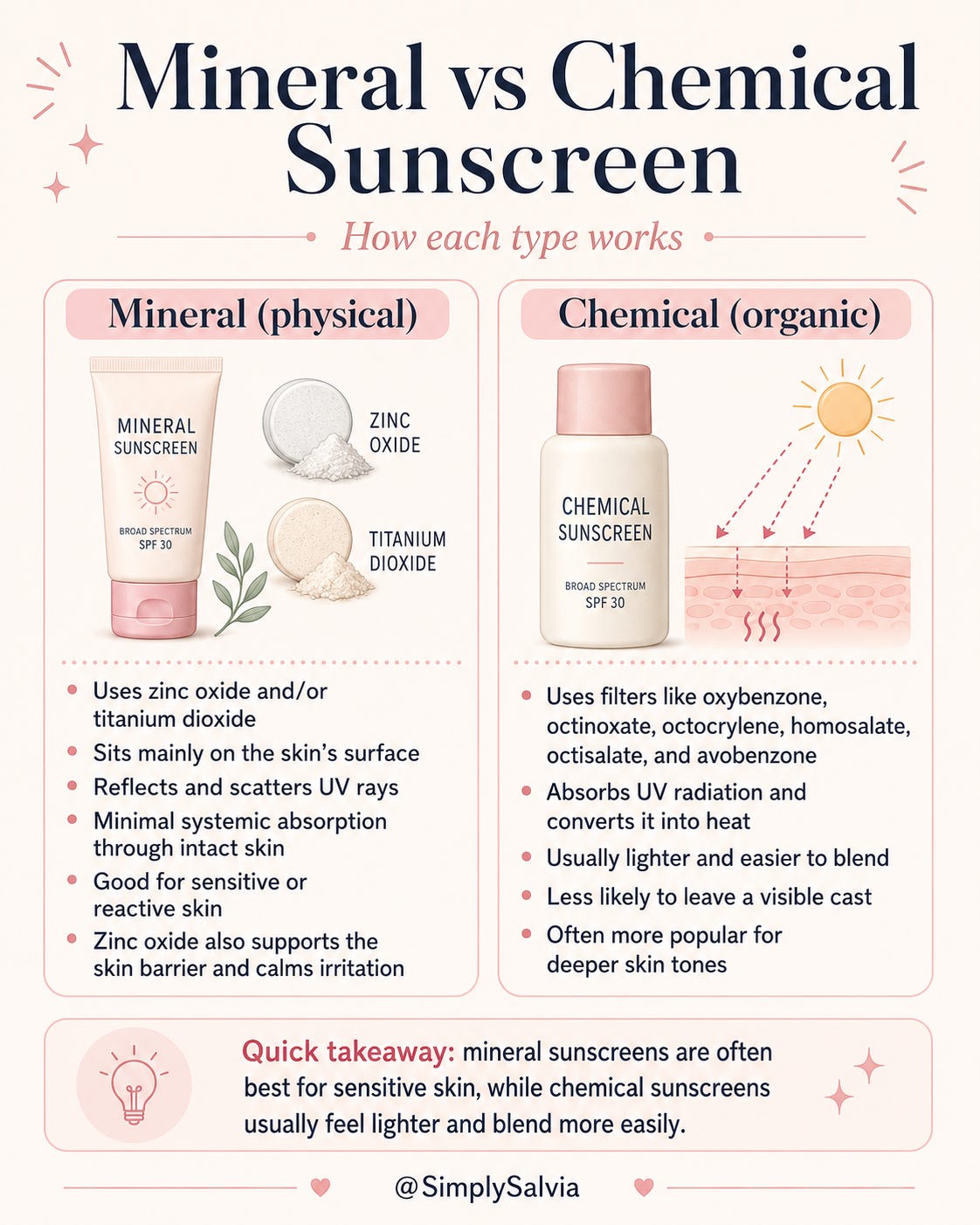
Mineral (physical) sunscreens use zinc oxide and/or titanium dioxide. These work primarily by sitting on the skin’s surface and physically reflecting and scattering UV radiation, rather than absorbing it into the skin. Studies using isotopically labelled zinc oxide have found minimal systemic absorption through intact human skin meaning very little of it enters the bloodstream. Zinc oxide also has independent anti-inflammatory and barrier-supportive properties, which is part of why it’s frequently recommended for sensitive or reactive skin.
Chemical (organic) sunscreens use compounds like oxybenzone, octinoxate, octocrylene, homosalate, octisalate, and avobenzone. These work by absorbing UV radiation and converting it to heat, which is then released from the skin. They tend to feel lighter, blend more easily, and are less likely to leave a visible cast, which has historically made them the more popular choice, particularly on deeper skin tones.
The Absorption Question: What 2026 Research Actually Shows
This is where the conversation has shifted meaningfully in the past few years, and it’s worth being precise rather than alarmist.
A 2019 FDA study found that several common chemical UV filters like oxybenzone, avobenzone, octocrylene, and others were absorbed into the bloodstream at levels significantly higher than previously understood, in some cases far exceeding the FDA’s own threshold for requiring further safety testing. A 2020 JAMA study found that a single day of using an oxybenzone-containing lotion produced plasma concentrations of 94.2 ng/mL, nearly 200 times the FDA’s 0.5 ng/mL threshold below which further testing typically isn’t required.
The important nuance: exceeding that threshold means the FDA wants more data, it does not automatically mean harm has been demonstrated. But the specific concern with oxybenzone has accumulated more weight over time. One fertility clinic cohort study found that higher oxybenzone levels were associated with lower antral follicle count in women under 35, and higher FSH (a hormone marker of declining ovarian reserve) in women over 35 suggesting a possible hormonal effect, though human research in this area remains limited and the clinical significance isn’t fully established. The National Toxicology Program also released findings linking oxybenzone exposure to increased thyroid tumour risk in female rats, and the European Commission’s safety review concluded oxybenzone is not considered safe at current permitted concentrations.
This research has had a real, measurable effect on the market: oxybenzone appeared in 70% of chemical sunscreens tested in 2016, and by 2026 that figure had dropped to just 5%, the industry has been actively reformulating away from it in response to the accumulating evidence, even ahead of any formal ban.
What This Means Practically, Without the Panic
The honest takeaway isn’t “chemical sunscreen is dangerous, switch to mineral immediately.” It’s more specific than that:
The strongest concern is specifically tied to oxybenzone, not chemical sunscreens as a category. If you check your sunscreen’s ingredient list and oxybenzone (sometimes listed as benzophenone-3 or BP-3) isn’t there, the absorption and hormonal concerns from the research above largely don’t apply to your product.
Some newer and more widely used in Europe chemical filters, bemotrizinol in particular have significantly better safety profiles, with minimal systemic absorption and no documented hormonal disruption concerns, and have been used safely across Europe, Asia, and Australia for over 20 years. The FDA approved bemotrizinol for use in the US for the first time in over two decades, with products expected to reach shelves in late 2026, a meaningful regulatory shift that’s been a long time coming.
Mineral sunscreen remains the most conservative choice for anyone wanting to minimise systemic absorption with the most established safety data, and is generally the first recommendation for sensitive skin, pregnancy, and younger users. The trade-off is cosmetic: mineral formulas can leave more of a visible cast, particularly on deeper skin tones, although tinted mineral formulas have improved significantly.
What’s not well supported by the evidence: avoiding sunscreen altogether because of these concerns. The documented risks of unprotected UV exposure; collagen breakdown, DNA damage, skin cancer risk are considerably better established and more serious than the absorption concerns around specific chemical filters. The right response to the oxybenzone research is switching to mineral sunscreen or a chemical sunscreen without oxybenzone, not abandoning sun protection.
Part 1 ends here. Part 2 covers exactly how much sunscreen to actually apply (the real-world gap is bigger than most people realise), how to balance sun protection with vitamin D, what to do if you’re acne-prone or dealing with pigmentation, the specific hormonal connection to melasma that almost no one explains properly, and the complete practical guide with product recommendations at every price point.
Now you understand what UV radiation is actually doing to your skin. The difference between UVA’s deep collagen damage and UVB’s surface-level burning and DNA damage, and why the visible effects show up years after the cellular damage begins. You know which myths are costing the most: the tan myth, the cloudy-day myth, the “higher SPF means less product” myth. And you have the current, nuanced picture on mineral versus chemical filters including the oxybenzone research specifically, rather than a blanket judgement on an entire category.
Part 2 turns all of this into something you can actually use.
Chapter 4 covers exactly how much sunscreen to apply and how often, including the research on just how large the real-world gap is between the SPF on the label and the protection most people are actually getting.
Chapter 5 is the vitamin D chapter. How to protect your skin without ending up deficient, and what the evidence actually supports as a reasonable middle ground.
Chapter 6 is specific to acne-prone, sensitive, and reactive skin, which formulas tend to work best and which ingredients to watch for.
Chapter 7 covers the hormonal dimension of sun damage that almost nobody explains properly: melasma, the menstrual cycle, and why pigmentation can worsen at specific hormonal points regardless of how diligent your SPF routine is.
Chapter 8 is the complete practical guide: product recommendations at every price point, the application cheat sheet, and the daily routine.
Subscribe to read Part 2 →
Sources & Further Reading
Early stage UV irradiation damage to skin collagen suppressed by HPA axis control — ScienceDirect
AAD: How to apply sunscreen — American Academy of Dermatology guidance
The Great Debate: Mineral vs Chemical Sunscreen — Dr. Heather Rogers, April 2026
What Sunscreen Is Safe? Mineral vs. Chemical Explained — ScienceInsights, April 2026
EWG’s Trouble with Sunscreen Chemicals report, 2026
EWG’s 20th Annual Guide to Sunscreens, May 2026
Dietary antioxidant intake in women with facial melasma — case-control study, October 2025