

Short Dive: The Acne Guide I Wish I’d Had at 16
It’s not just about your skincare routine. Here’s what the research actually says about why you break out, and what actually fixes it.

I had acne for about seven years before I understood what was actually happening in my skin.
Not the vague “hormones” explanation. Not “you need to drink more water.” The actual mechanism. The biology. The reason certain weeks are reliably worse than others. The reason the cleanser that’s supposed to “clear pores” sometimes makes things worse. The reason the expensive serum did nothing while the cheap tube from the pharmacy did something.
Nobody told me any of it. Not the GP. Not the dermatologist I waited four months to see. And definitely not the TikTok comments.
So this short dive is the explanation I didn’t get at 16. What acne actually is, why your hormones are involved in more ways than you probably realise, what the evidence hierarchy actually looks like for treatment, and the practical guide that puts all of it together.
Let’s start at the beginning.
What Acne Actually Is And Why Most People Are Fighting It Wrong
Why Your Hormones Are Running the Show — The Menstrual Cycle and Your Skin
Chapter 1: What Acne Actually Is And Why Most People Are Fighting It Wrong
The Four-Step Mechanism
Acne isn’t caused by dirty skin. It isn’t caused by not washing your face enough. And it definitely isn’t caused by touching your face. These ideas have been so thoroughly embedded in the way we talk about breakouts that they’ve produced an entire generation of people over-cleansing, over-exfoliating, and stripping their skin barrier in the name of treating acne, which, as I’ll get to, actively makes acne worse.
Here’s what’s actually happening.
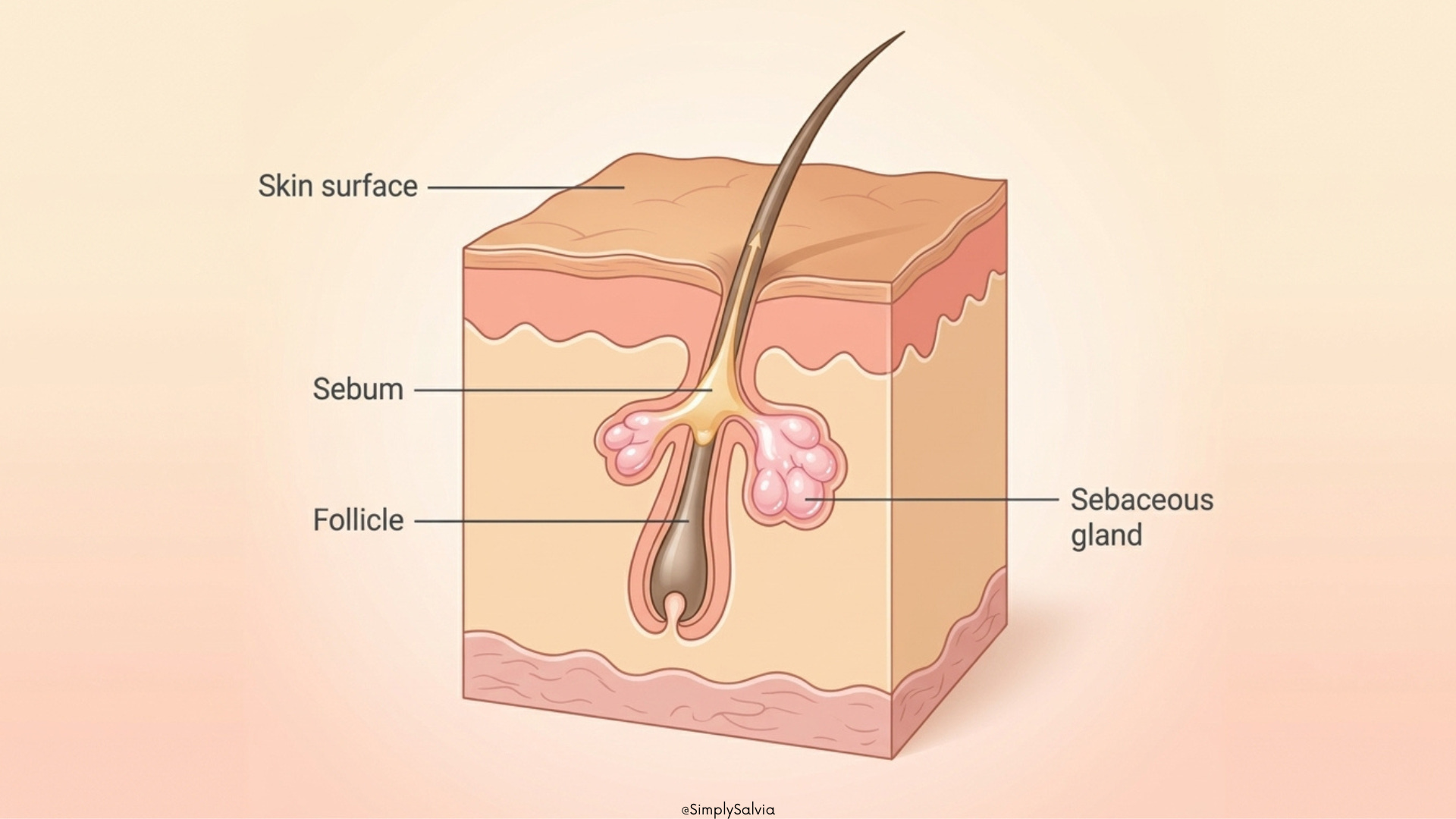
Inside each of your pores is a hair follicle with an attached sebaceous gland; a tiny oil-producing structure. Your sebaceous glands produce sebum, which is the oil that keeps your skin lubricated and barrier-protected. This is not a bad thing. Sebum is a normal, necessary part of skin function.
Acne happens when four things go wrong in sequence inside these pores:
Step 1: Too much sebum. The sebaceous gland produces more oil than the follicle can handle. Androgens, specifically dihydrotestosterone (DHT), a form of testosterone, are the main driver of this. More androgen activity means the gland works harder and produces more sebum. This is why acne is so common in puberty (androgens surge), why it’s connected to the menstrual cycle (androgen levels fluctuate relative to estrogen), and why it’s often worse in the premenstrual week.
Step 2: The pore gets blocked. The skin cells that line the inside of the follicle normally shed naturally and exit through the pore. When they don’t, when they build up and stick together instead of exiting they form a plug. This blockage is called a comedo. A comedo that stays closed under the skin is a whitehead. One that opens at the surface and oxidises (turns dark on contact with air) is a blackhead. The dark colour is not dirt. It’s oxidised sebum and skin cells.
Step 3: Bacteria multiply. A bacterium called Cutibacterium acnes (C. acnes) lives on everyone’s skin all the time. It’s part of a healthy skin microbiome. The problem is that C. acnes loves the environment inside a blocked, sebum-filled follicle. It feeds on the sebum, multiplies rapidly, and in doing so breaks down the sebum into free fatty acids that are irritating to the follicle wall.
Step 4: Inflammation. Your immune system detects the bacterial activity and sends inflammatory signals to the area. This is what turns a blocked pore into a red, raised, painful spot. The inflammation can be mild (a small red papule), moderate (a pus-filled pustule), or severe (a deep, painful cyst or nodule that sits under the skin and never comes to a head).
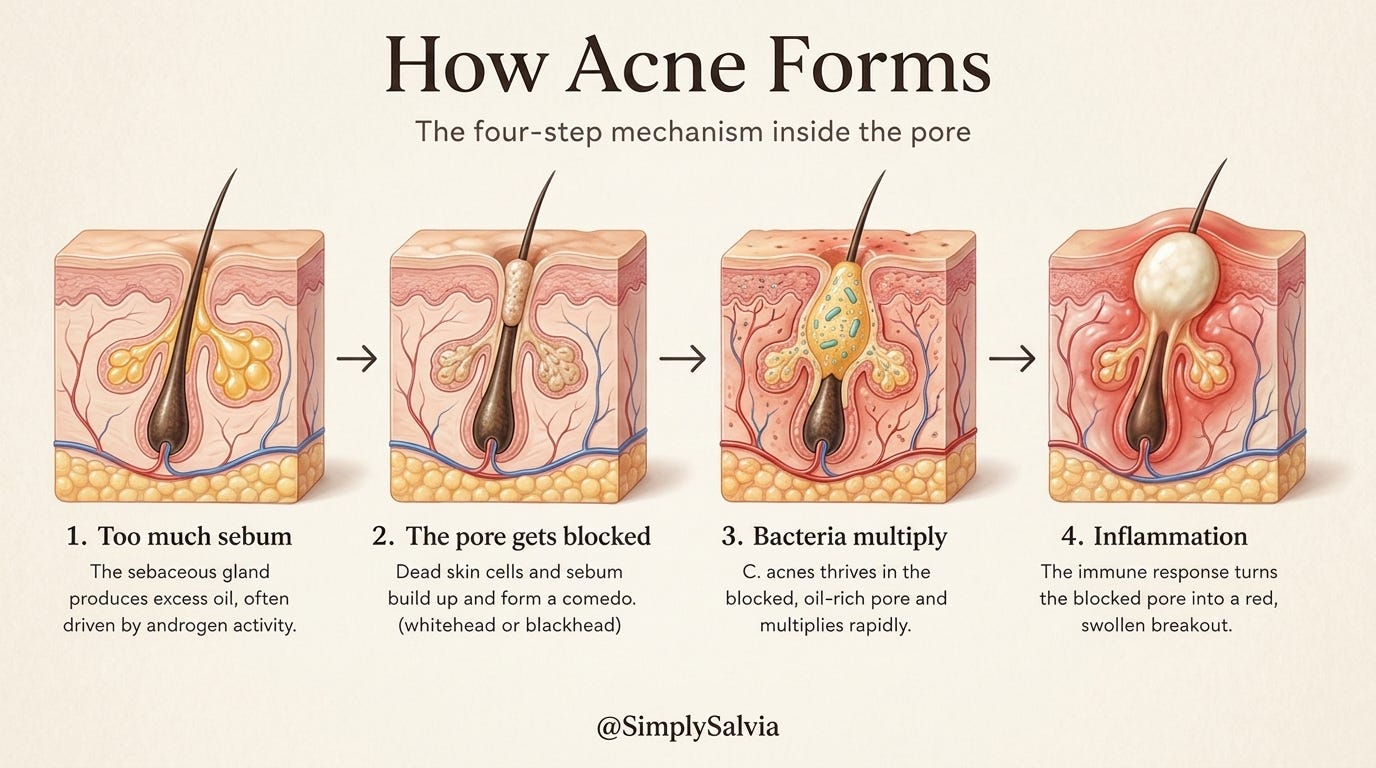
This four-step process — excess sebum, blocked pore, bacterial growth, inflammation, is the foundation of all acne. Understanding it explains why specific treatments work: retinoids target the blocked pore step, benzoyl peroxide targets the bacterial step, anti-inflammatory ingredients and hormonal treatments target the sebum step upstream.
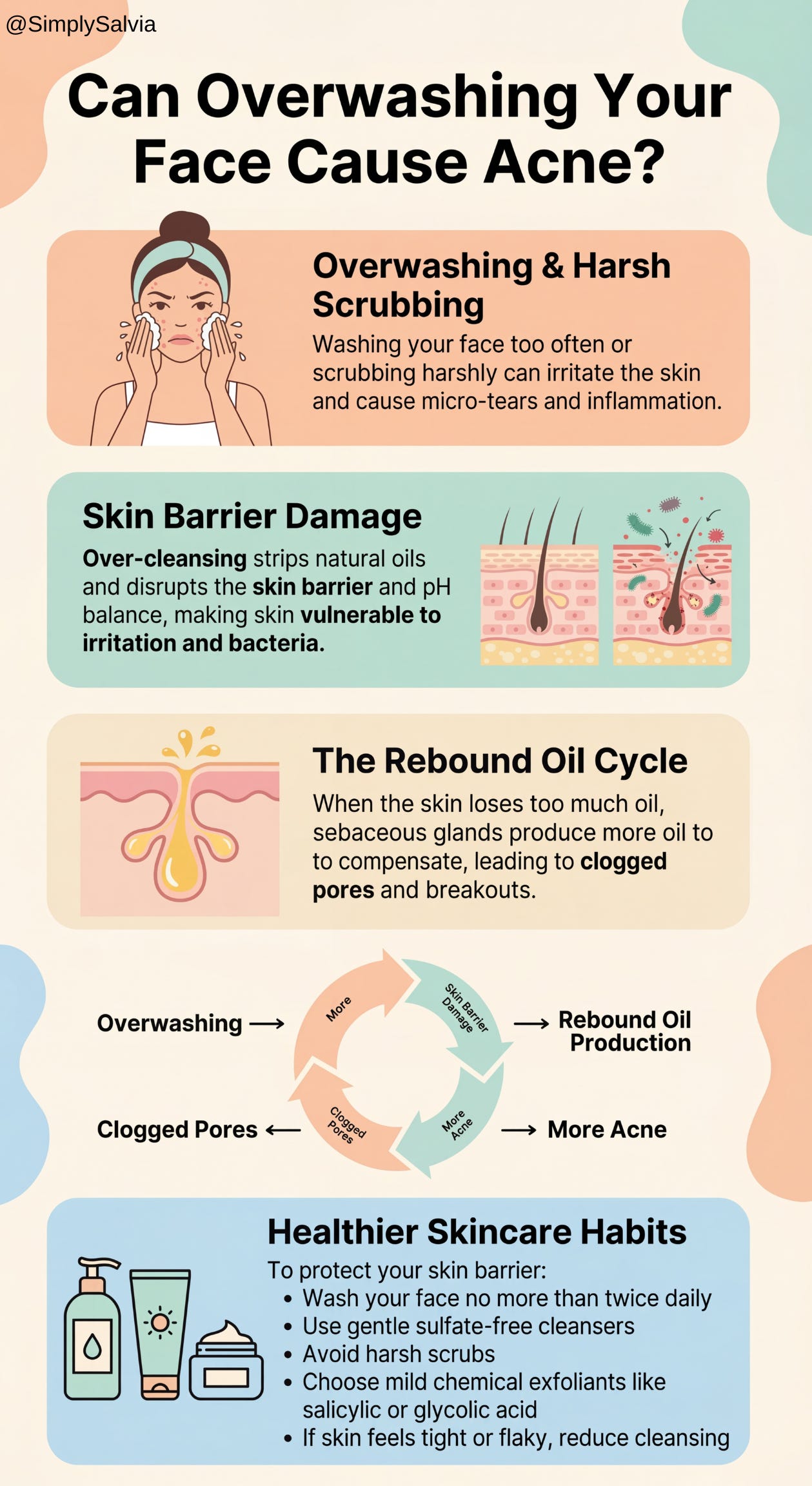
Why Washing Your Face More Makes It Worse
Here’s the part that matters practically: harsh cleansing, over-exfoliation, and stripping products — the instinctive response to oily, broken-out skin, all damage the skin barrier.
A damaged skin barrier makes acne worse in two ways. First, it triggers an inflammatory response that is the same pathway as the inflammatory acne response. Second, it signals the skin to produce more sebum as a compensatory repair mechanism. So stripping your skin makes it oilier and more inflamed which is the exact opposite of what you’re trying to achieve.
A December 2025 review in Molecules covering over 100 acne sources confirmed that maintaining the skin barrier is now considered a critical component of acne management and not just a nice-to-have alongside active treatments.
The correct cleansing approach for acne-prone skin: a gentle, non-foaming or low-foam cleanser, twice a day maximum, that removes surface excess without stripping. That’s it. The work of treating acne happens with the treatments applied after cleansing, not with the cleanser itself.
Chapter 2: Why Your Hormones Are Running the Show — The Menstrual Cycle and Your Skin
This is the chapter that most acne content skips entirely, or covers in one vague sentence about “hormonal acne.” The biology is more specific than that, more interesting than that, and more useful than that because once you understand which hormones do what in which week, the monthly breakout pattern that felt random starts to make complete sense.
The Phase-by-Phase Skin Picture
Your skin contains receptors for estrogen, progesterone, and androgens. Which means every hormonal shift across your cycle is being detected and responded to in your skin and not just in your mood or your sleep.
Week 1 — Menstrual phase: Both estrogen and progesterone are at their lowest. Skin is often in a post-breakout recovery phase. The barrier can be more reactive than usual because prostaglandins (which drive cramping) also affect the skin’s inflammatory state. Sebum production is lower in this phase.
Week 2 — Follicular phase: Estrogen is rising. Estrogen has a genuinely beneficial effect on skin: it supports the skin barrier, promotes collagen synthesis, and critically, reduces sebum production. As estrogen rises through the follicular phase, skin tends to clear and brighten. Many women notice their skin looks best in the week after their period ends. This is why.
Around ovulation: Estrogen peaks, and with it comes the clearest, most luminous skin of the month for many women. But this is also when a brief testosterone surge occurs alongside the LH spike that triggers egg release. For women with more androgen-sensitive sebaceous glands, this can trigger a small breakout right around ovulation even when the rest of the month is clear.
Weeks 3–4 — Luteal phase: This is where things get more complicated. After ovulation, progesterone rises and becomes the dominant hormone. Progesterone stimulates the sebaceous glands to produce more oil. At the same time, as estrogen falls in the late luteal phase, its sebum-suppressing effect disappears. And androgens, still present throughout the cycle become relatively more dominant as estrogen drops.
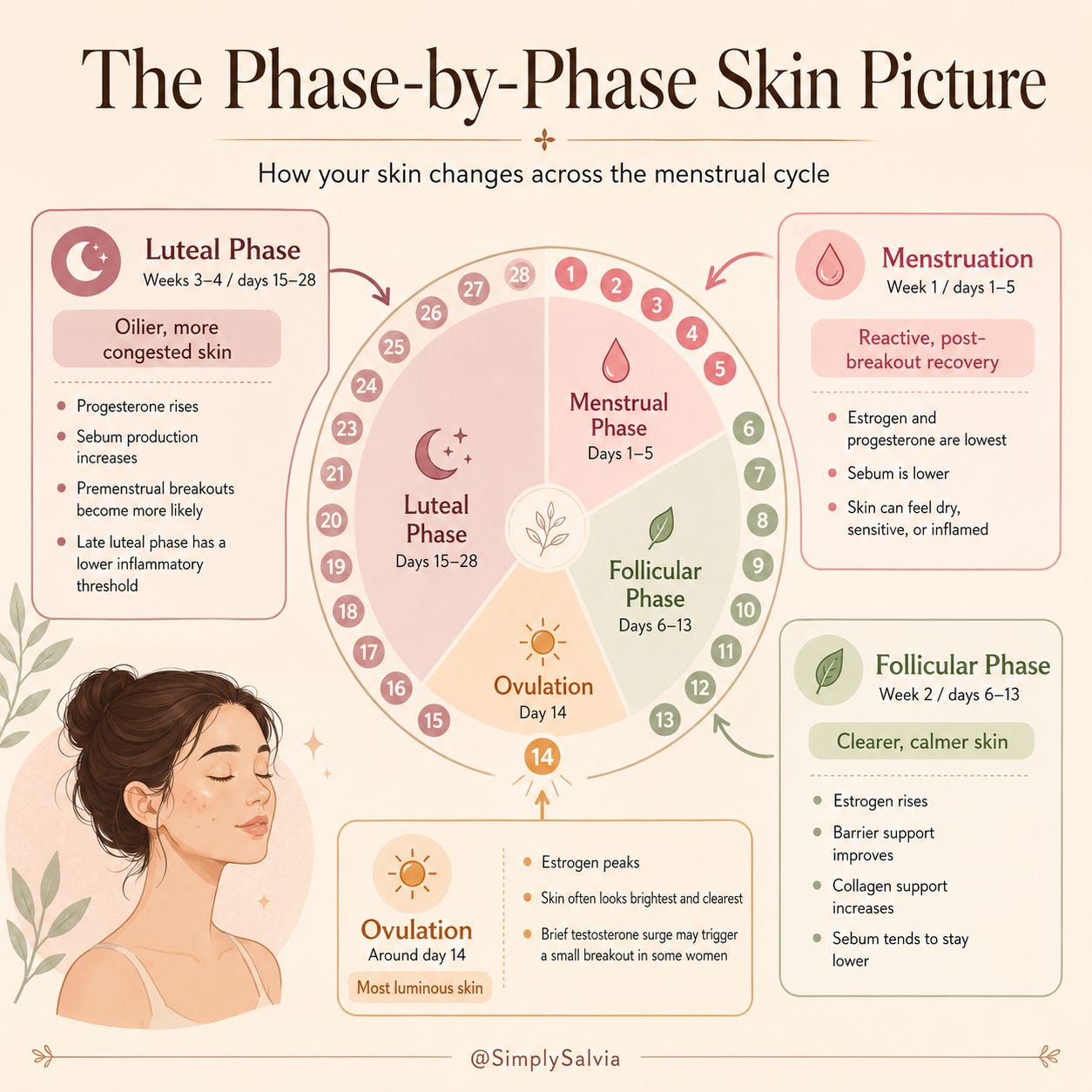
The result: sebum production peaks in the premenstrual week. The follicular environment is oilier, the conditions for bacterial growth are better, and the inflammatory threshold is lower because the late luteal phase is already a time of heightened systemic inflammation. A 2025 study published in The Journal of Dermatology found that sebum composition changes measurably across the menstrual cycle, with the luteal phase showing the most significant shifts in the lipid profile that drives C. acnes activity.
Approximately 65% of women report worse breakouts in the week before their period. The hormonal explanation is real, documented, and explains exactly why.
Where Hormonal Acne Shows Up and Why
The location of acne breakouts is not random. It’s connected to the density and sensitivity of sebaceous glands in specific areas, and to the hormonal pathways driving them.
Hormonal acne has a signature location: the lower third of the face. Jawline, chin, and the area around the mouth. These are the areas with the highest concentration of androgen-sensitive sebaceous glands aka the glands that respond most to DHT. When androgens drive excess sebum production, this is where it shows up first.
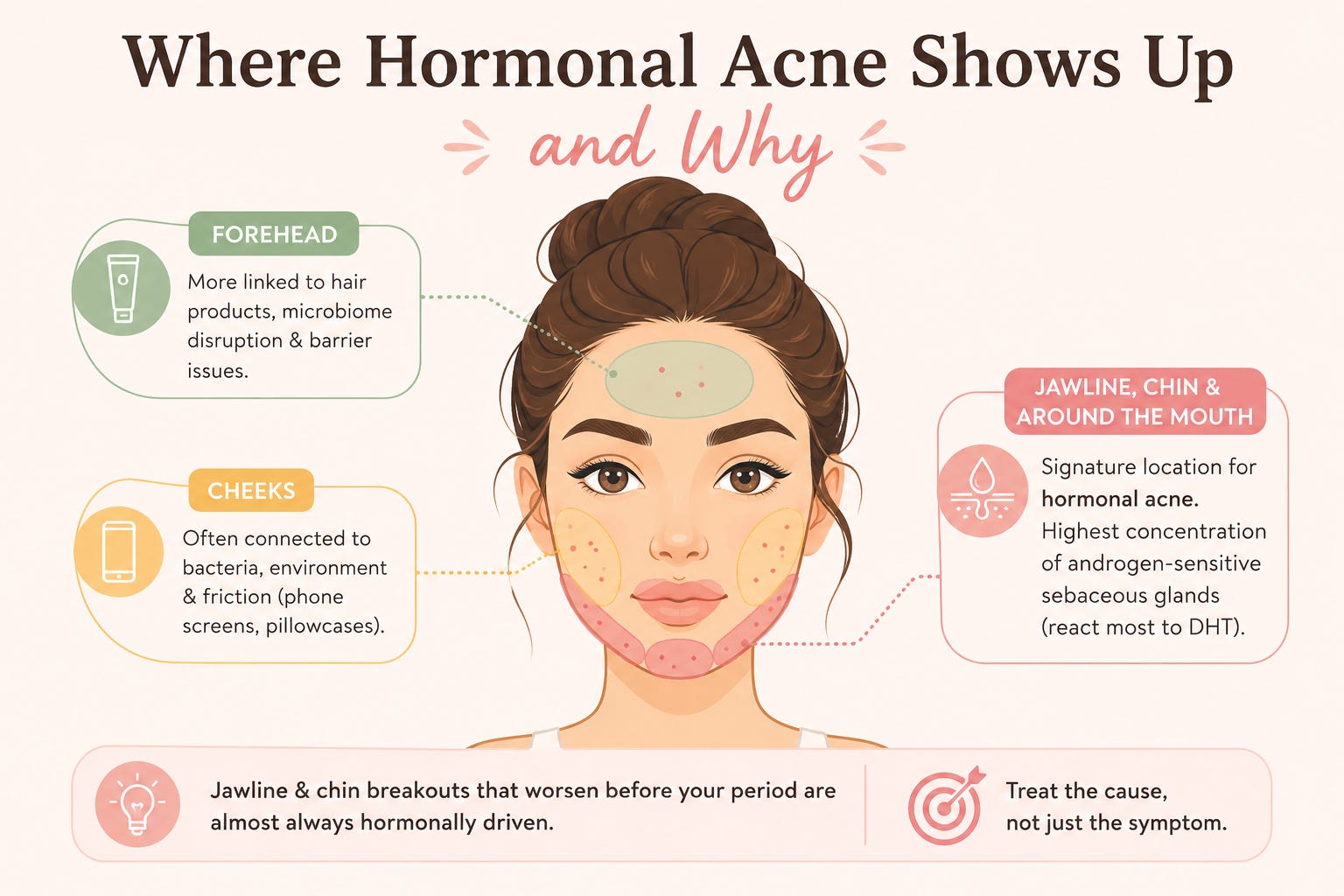
Forehead acne tends to be more connected to skin microbiome disruption, hair products, and barrier issues than to hormones. Cheek acne often has a bacterial, environmental, or friction component (phone screens, pillowcases). Jawline and chin acne that reliably worsens in the week before your period is almost always hormonally driven, which means treating it purely topically, while not addressing the hormonal environment driving it, is treating the symptom rather than the cause.
The Gut-Estrobolome-Jawline Connection
This is the link that’s gaining research attention and that almost no skincare content is discussing yet.
As covered in Between Saturdays, the estrobolome (the collection of gut bacteria responsible for metabolising estrogen) plays a direct role in how much estrogen circulates in the body. When gut microbiome diversity is low, estrogen clearance is impaired. Estrogen that should be processed and excreted stays in circulation longer. Elevated estrogen levels relative to progesterone create a hormonal environment that can worsen acne through several pathways, including by suppressing testosterone-binding proteins, which effectively raises free androgen activity in the skin.
A 2025 review in Dermatology Research and Practice confirmed that the gut-skin axis is now considered a significant factor in acne pathogenesis and that gut microbiome composition is measurably different in people with acne compared to those without it.
This is why for some women, persistent hormonal acne, especially the jawline cystic kind that doesn’t fully respond to topical treatment has a gut health component. The dietary pattern that most consistently supports the estrobolome and reduces the gut-skin inflammatory pathway: high-fibre eating from varied plant sources, fermented foods, reduced ultra-processed food. The same pattern that supports gut health generally.

Chapter 3: The Evidence Hierarchy — What the Research Actually Ranks
This is the chapter where I tell you that most of what wellness TikTok recommends for acne is not at the top of the evidence hierarchy and what actually is.
The American Academy of Dermatology’s 2024 Guidelines
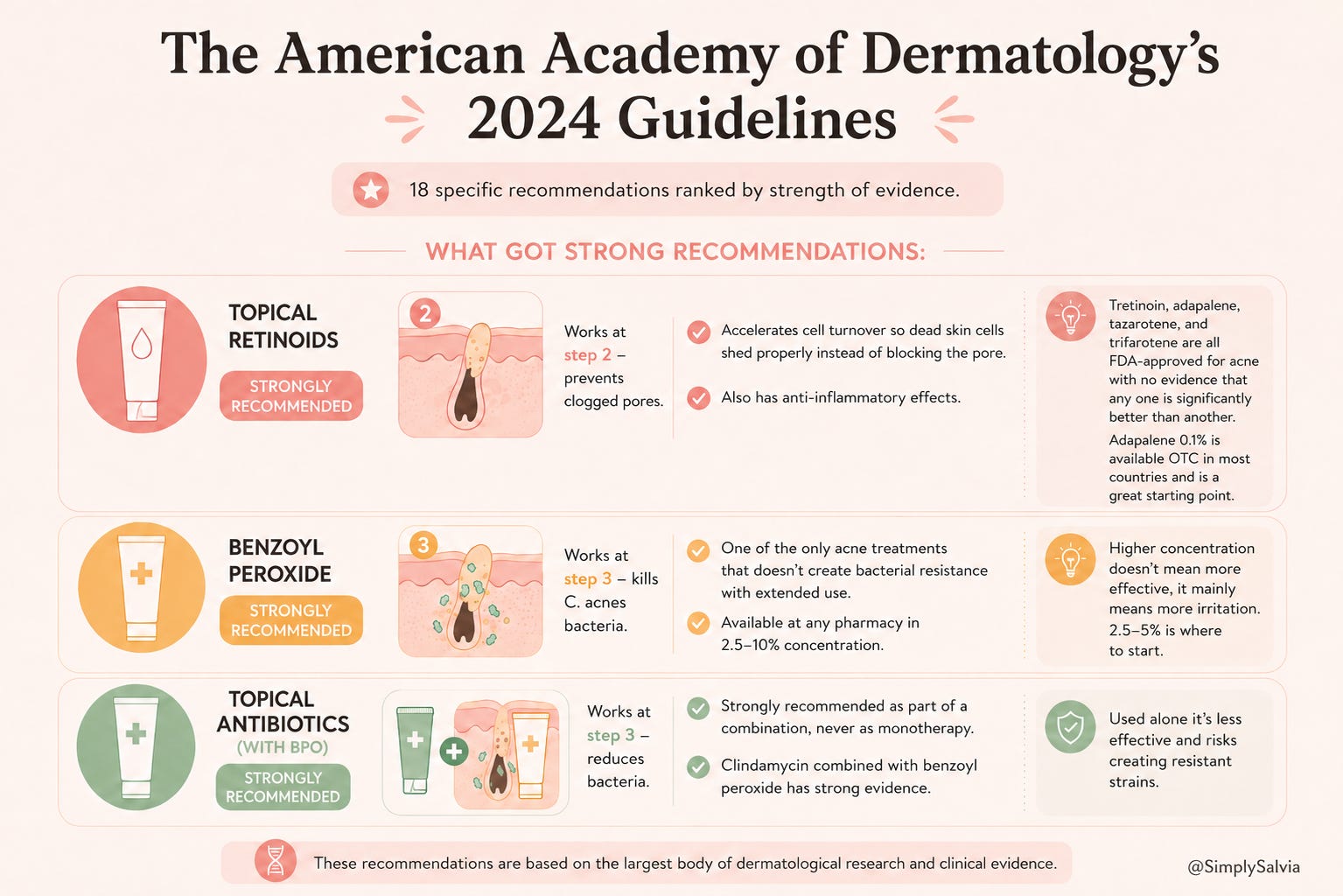
The AAD published updated clinical guidelines for acne management in 2024. These are evidence-based recommendations from the largest body of dermatological research. 18 specific recommendations ranked by strength of evidence. Here’s what got strong recommendations:
Topical retinoids. Strongly recommended. Work at step 2 of the acne mechanism. They accelerate cell turnover so the dead skin cells that form the follicular plug shed properly rather than building up and blocking the pore. They also have anti-inflammatory effects. Tretinoin, adapalene, tazarotene, and trifarotene are all FDA-approved for acne, with no evidence that any one is significantly better than another. Adapalene 0.1% is available over the counter in most countries and is a genuinely effective starting point.
Benzoyl peroxide. Strongly recommended. Works at step 3 — it kills C. acnes bacteria. Notably, it’s one of the only acne treatments that doesn’t create bacterial resistance with extended use (unlike antibiotics). Available at any pharmacy at 2.5–10% concentration. Higher concentration doesn’t mean more effective, it mainly means more irritation. 2.5–5% is where to start.
Topical antibiotics (with BPO). Strongly recommended as part of a combination, never as monotherapy, because antibiotic resistance is a real concern with acne bacteria. Clindamycin combined with benzoyl peroxide has strong evidence. Used alone it’s less effective and risks creating resistant strains.
What got conditional recommendations (real but not the strongest evidence):
Salicylic acid. A beta-hydroxy acid that exfoliates inside the pore. Useful for non-inflammatory, comedonal acne (blackheads and whiteheads). Less effective for inflammatory spots. A good addition but not a first-line treatment for inflammatory acne.
Azelaic acid. Antibacterial and anti-inflammatory, and has the additional benefit of reducing post-inflammatory hyperpigmentation, the dark marks left after spots. Excellent for darker skin tones where PIH is a significant concern. Evidence is real but thinner than for retinoids or BPO.
Niacinamide. Not in the AAD guidelines as a primary acne treatment but has research support for reducing sebum production and skin inflammation. Works as a supporting ingredient rather than a primary treatment.
What Didn’t Make the Evidence Hierarchy
Tea tree oil. Some evidence for mild antibacterial effects, but not at a level that competes with the above. Useful for very mild, occasional breakouts. Not a treatment for inflammatory acne.
Hypochlorous acid. Trending at 132% YoY search growth in 2026. Genuinely useful as it kills C. acnes without creating resistance and is extremely well tolerated by sensitive and compromised skin barriers. But: the acne evidence is thinner than the eczema and wound-healing evidence, and the AAD guidelines don’t include it as a primary treatment. It belongs in a routine, but it’s not doing the heavy lifting.
Natural alternatives generally. Witch hazel, apple cider vinegar, lemon juice, none of these have evidence comparable to the treatments above. Apple cider vinegar and lemon juice can actively damage the skin barrier and should not be applied directly to the face.
Supplements marketed for skin. Zinc has the most interesting acne evidence, it has some anti-inflammatory and antibacterial properties and several studies have found it reduces inflammatory lesion count. But even zinc’s evidence is modest compared to topical retinoids. Supplements sit at the bottom of the evidence hierarchy for acne treatment, not the top.
Why the Evidence Hierarchy Matters
The reason most people cycle through product after product and don’t get consistent results is that they’re investing money and time in ingredients at the bottom of the evidence hierarchy (trendy, gentle, wellness-adjacent) while avoiding or misusing the ingredients at the top (retinoids, BPO) because they’re less aesthetically appealing, require a learning curve, or are just less well marketed.
Adapalene 0.1% costs less than most trendy serums. It has strong evidence behind it. It’s available without a prescription in most countries. The reason it’s not on TikTok every week is that you can’t make it in a pretty bottle with a compelling brand story — the patent expired decades ago.
That’s not a knock on the skincare industry. It’s useful information for where to put your attention and your money.
Part 1 ends here. Part 2 is the practical half. The ingredient guide, the routine, the diet chapter, the hormonal acne protocol, and the phase-by-phase skincare guide for the weeks where breakouts are reliably worse.
Now you know more about what’s actually happening in your skin than most skincare content will ever tell you. You know the four-step mechanism. You know how estrogen, progesterone, and androgens play out across the month and why the premenstrual week is reliably the hardest. You know that the gut microbiome is involved in hormonal acne in a specific way that most people aren’t talking about. And you know what the evidence hierarchy actually looks like, which treatments are strongly recommended, which are conditionally recommended, and which are mostly marketing.
Part 2 is where it becomes a system you can actually use.
Chapter 4 is the ingredient deep dive. How each of the evidence-backed ingredients works, which skin types they suit, and what concentration to start with. Including the honest assessment of hypochlorous acid, azelaic acid, and niacinamide and where they actually belong in a routine.
Chapter 5 is the diet chapter. What the research genuinely supports for acne and skin. The glycaemic index evidence is stronger than most people know. The dairy evidence is more nuanced than most people have been told. The omega-3 finding will probably surprise you.
Chapter 6 is how to build a routine that treats acne without destroying your barrier in the process, because the most common reason acne treatments don’t work is the over-treating that compromises the very barrier you need intact.
Chapter 7 is the hormonal acne protocol. Specific, phase-aware adjustments for the week before your period when the sebum-androgen-inflammation picture is at its most difficult.
Chapter 8 is the complete practical guide: a simple, evidence-based routine from cleanser to SPF, shopping suggestions at different price points, and the signs that mean your acne needs a GP or dermatologist rather than a product change.
Subscribe to read Part 2 →
Sources & Further Reading
MDPI Biomolecules. The Evolving Microbial Paradigm in Acne — March 2026
Menstrual cycle phases and acne flares — ScienceDirect, September 2025
Healthline. Period acne guide — updated January 2026
AAD Guidelines of care for the management of acne vulgaris — JAAD, January 2024
Systematic review: low glycaemic load diets and acne, 2025
Löffler et al. Deficit of omega-3 fatty acids in acne patients — PMC, 2024
La Belle Vie. Acne treatment trends 2026 — hypochlorous acid and emerging ingredients
Skin Science Hub. Hypochlorous acid for skin — December 2025