

Deep Dive: High Blood Pressure Isn’t Just an Older Person’s Problem (Part 1)
The condition your parents worry about is quietly showing up in women your age. Most of them have no idea. Here's everything you need to know — starting with why you should care at 20.

She was 24. A postgraduate student. Tired, headachy, running on coffee and deadlines — but nothing that felt unusual for the life she was living. She went to the GP for something unrelated. A prescription, a check-up, nothing significant.
The nurse took her blood pressure at the start of the appointment and paused.
Took it again. Paused again.
Her reading was 158/102.
Stage 2 hypertension. In a 24-year-old who exercised, didn’t smoke, didn’t feel unwell, and had no family history she knew of. Who would have gone home that day without the reading ever being taken, continued feeling fine, and had no idea that the pressure inside her arteries was high enough to be quietly damaging her heart, her kidneys, and her brain.
This is the thing about high blood pressure. It doesn’t feel like anything. It is the most common cardiovascular condition in the world, and it gives you almost no warning that it’s there.
I know what you’re thinking. Blood pressure is an old person’s problem. I’m 20. I eat reasonably, I’m not particularly unwell. Why does this apply to me?
Here’s why.
1 in 5 women aged 18 to 39 in the US currently has hypertension. Not 1 in 5 people in their 60s. Women. Our age. Right now. And 73% of young adults who have it have no idea — because it produces no symptoms, nobody checks at this age, and everyone assumes it’s a problem for later.
The American Heart Association published a scientific statement in early 2026 with a projection that stopped me when I read it: by 2050, nearly 1 in 3 women aged 22 to 44 are expected to have some form of cardiovascular disease. High blood pressure is the primary driver of that number. The women accumulating that risk aren’t in their 50s. They’re accumulating it now — in their 20s and 30s — while being told not to worry about it yet.
The problem with “worry about it later” is what happens in the gap.
High blood pressure doesn’t announce itself and then cause damage. It is the damage — building silently in the walls of your arteries, the muscle of your heart, the microvasculature of your brain and kidneys, for years before anything becomes visible or symptomatic. By the time a reading catches up with you, the question isn’t whether to prevent it. It’s how much has already accumulated.
Here’s what else I didn’t know until I went looking: women’s blood pressure starts rising faster than men’s from around age 20 onwards. Not from menopause. From now. The cardiovascular protection that oestrogen provides is real — but it doesn’t mean your blood pressure is staying flat while you coast through your 20s. The trajectory starts earlier than most women are ever told.
And it’s not just genetics or fate. Chronic stress activates the same hormonal pathways that raise blood pressure. Sleep deprivation disrupts the overnight drop in BP that healthy arteries depend on. Ultra-processed food erodes the sodium-potassium balance that keeps vascular tone in check. The oral contraceptive pill raises blood pressure in some women — and the ones most at risk often don’t know to ask. Every one of these things is more characteristic of being 22 than 62. The risk factors are not abstract. They are Tuesday.
I went down this rabbit hole because a close friend had a reading she couldn’t explain, and I realised neither of us knew anything real about what blood pressure actually was — how it worked, what drove it, and what a person our age could actually do about it. The standard advice felt hollow: cut salt, exercise more, relax. We’d heard it. It didn’t tell us anything we could use.
So I went to the research instead. What I found is that this is a topic that deserves to be understood at the systems level — not just as a number to keep below a threshold, but as a reflection of how your nervous system, hormones, kidneys, and vascular health are functioning together. And when you understand it that way, the interventions that actually work start to make a lot more sense.
This is the guide I wish existed before I started looking into this properly.
Here’s what this Deep Dive covers:
Section 1: The Silent Killer You Don’t Feel — Until It’s Too Late
Why Your Body Pushes Blood Pressure Higher — And Keeps It There
The Minerals Your Diet Is Missing That Are Quietly Raising Your Blood Pressure
You Can Feel Completely Fine and Still Have Dangerously High Blood Pressure
What Happens at the Doctor and What Those Numbers Actually Mean
Normal, Elevated, Stage 1, Stage 2: Where Do Your Numbers Actually Fall
Hope you enjoy reading and learning with me, Simply Salvia
PS: We also have a subscriber-only group chat where members discuss the deep dives, share their sleep journeys, and ask me questions directly. See you there.
Disclaimer: The information and opinions expressed above are current as of the date of this post and are subject to change without notice. Materials referenced above are provided for educational and informational purposes only. None of the above constitutes medical advice, a diagnosis, a treatment recommendation, or a substitute for consultation with a qualified healthcare professional. Always seek the guidance of your doctor or another qualified health provider with any questions you may have regarding a medical condition or sleep disorder.
Deep Dive below ↓
Section 1: The Silent Killer You Don’t
Feel — Until It’s Too Late
1. What Is Blood Pressure and What Does “High” Actually Mean?
Blood pressure is a measure of the force your blood exerts against artery walls as your heart pumps. High blood pressure (or hypertension) is a condition where the force of blood against the artery walls is consistently too high. It’s expressed in two numbers:
Systolic (pressure when the heart contracts) and
Diastolic (pressure when the heart rests between beats).
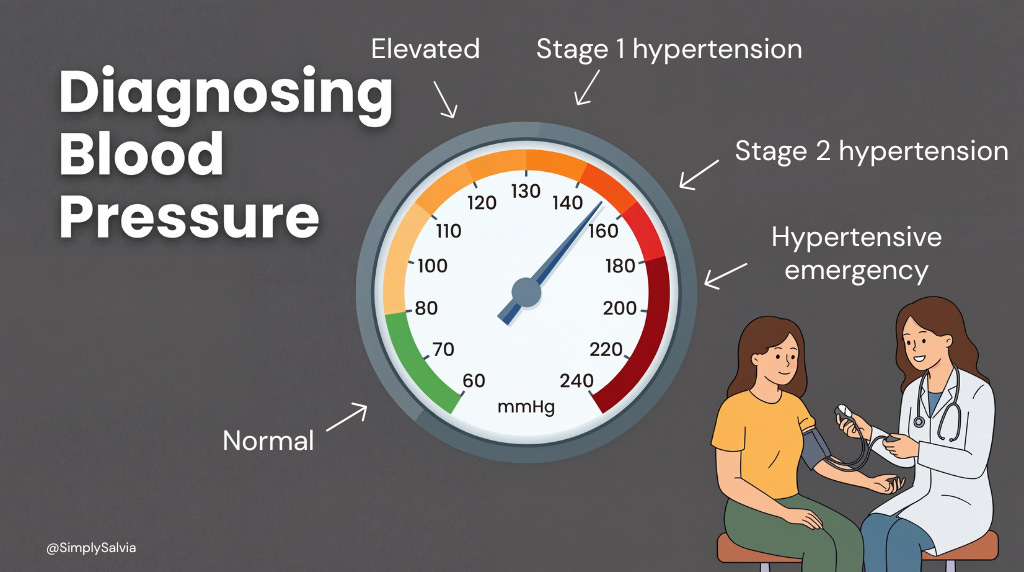
For example, a normal reading like 118/76 mmHg means a systolic of 118 and a diastolic of 76. Hypertension according to ACC/AHA guidelines, the categories break down like this:
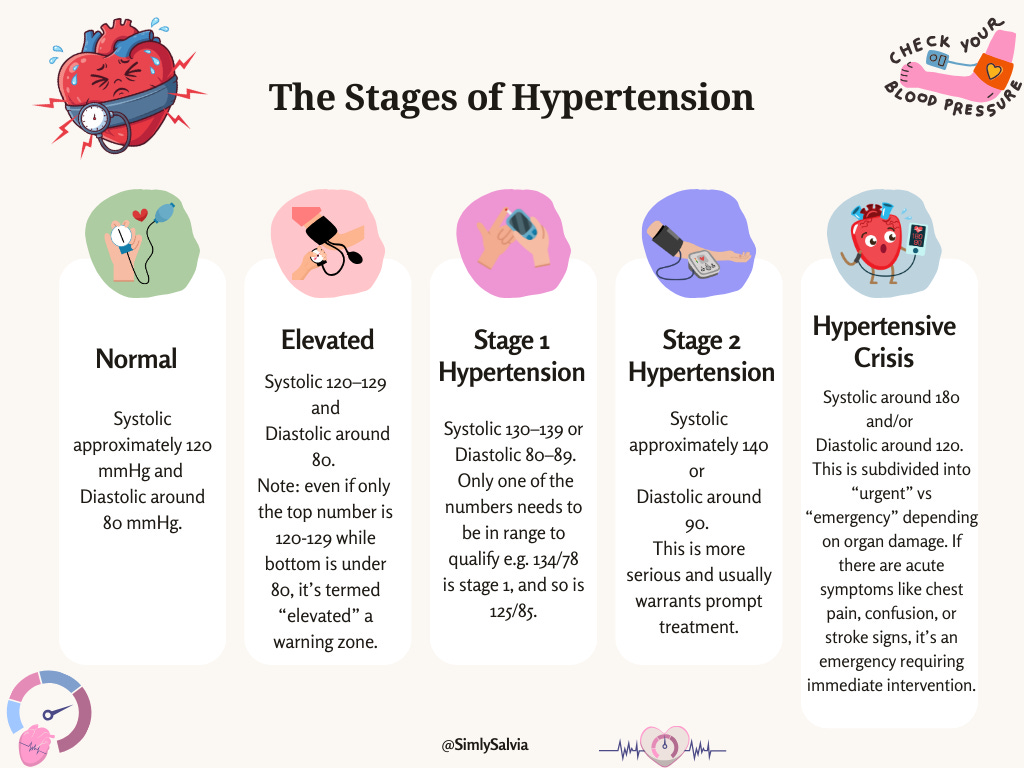
Under 120/80: Normal — maintain healthy habits
120–129/under 80: Elevated — not yet hypertension, but worth acting on
130–139/80–89: Stage 1 hypertension — lifestyle changes and possibly medication depending on risk
140/90 or above: Stage 2 hypertension — medication likely recommended alongside lifestyle changes
180/120 or above: Hypertensive crisis — requires immediate medical attention
It’s often called the “silent killer” because most people feel no symptoms even when blood pressure is dangerously high. This silent nature makes hypertension a silent epidemic, millions have it unknowingly. The WHO’s 2025 global hypertension report estimates that 1.4 billion adults worldwide currently live with hypertension — yet fewer than one in five have it adequately controlled. Over time, uncontrolled high blood pressure quietly damages blood vessels and vital organs. This is why hypertension is so dangerous without symptoms: by the time headaches, dizziness, or other signs occur, serious damage may have already taken place. Early detection through routine blood pressure checks is crucial. Simply put: hypertension is common, often invisible, but very serious if untreated.
2. Why Your Body Pushes Blood Pressure Higher — And Keeps It There
Primary (essential) hypertension accounts for about 90–95% of cases and has no single identifiable cause. It develops from a mix of genetic factors and lifelong habits. As we age, our arteries naturally stiffen and may narrow due to cholesterol plaque leading to increased pressure. The renin–angiotensin–aldosterone system (RAAS) plays a key role: it’s the body’s hormone system for regulating blood volume and vessel tone. When blood pressure falls, the kidneys release renin, which triggers production of angiotensin II, a hormone that constricts blood vessels and stimulates aldosterone release. Aldosterone causes the kidneys to retain sodium (and thus water), increasing blood volume.
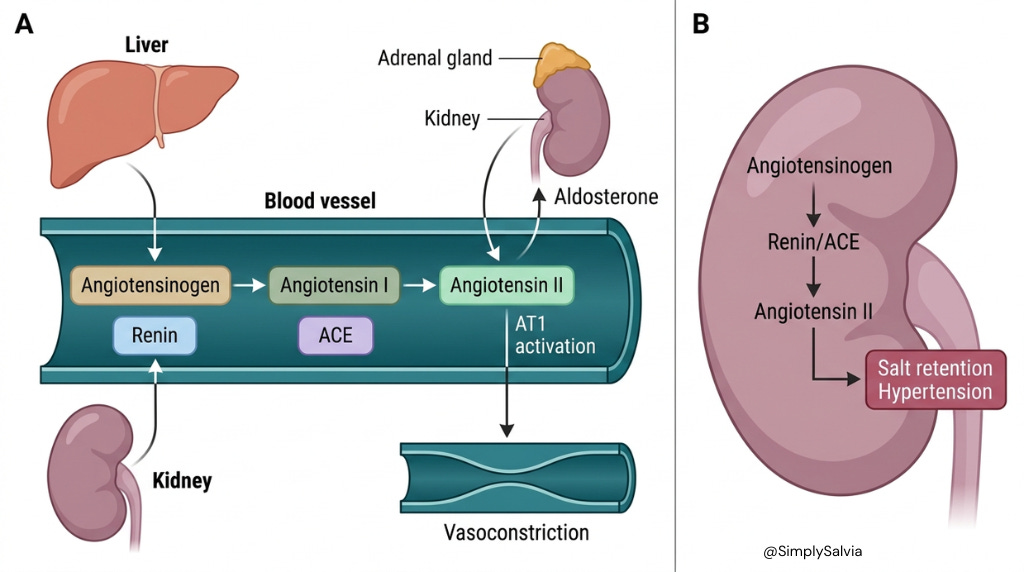
In hypertension, RAAS can become overactive causing chronic vasoconstriction and fluid retention that drive blood pressure up. The sympathetic nervous system (the “fight or flight” response) may also be in overdrive, keeping heart rate and vessel tone higher than normal. Even the kidneys themselves influence pressure set-points by controlling how much sodium and water the body holds onto. In some people, the kidneys require a higher pressure to excrete salt, effectively “resetting” blood pressure to a high level.
Meanwhile, secondary hypertension (5–10% cases) results from an underlying condition. Common causes include kidney diseases; like chronic kidney disease or renal artery narrowing, endocrine disorders, and others (I’ll explore these in Section 8). In any case, hypertension usually arises from a combination of factors: the blood vessels may constrict or harden thus raising resistance, the heart may pump harder or faster, the kidneys may retain too much fluid, and the nervous/hormonal systems may overstimulate pressure. Think of blood pressure like water in a hose: narrowing the nozzle (vasoconstriction) or turning up the faucet (blood volume) will increase the pressure. Hypertension often involves both; tighter vessels and higher fluid volume.
The renin-angiotensin system exemplifies this dual effect. Angiotensin II tightens arteries and also leads to more fluid retention via aldosterone. Over time, these mechanisms become maladaptive. The result is chronically elevated pressure that makes the heart and vessels work overtime. Primary hypertension tends to develop gradually over years, influenced by lifestyle (diet, exercise, stress) and genetic predispositions. It is complex, but understanding these basics, vessel tone and fluid volume gives insight into why treating hypertension often requires a multifaceted approach e.g. medications that relax vessels or help the body shed water.
3. The Minerals Your Diet Is Missing That Are Quietly Raising Your Blood Pressure
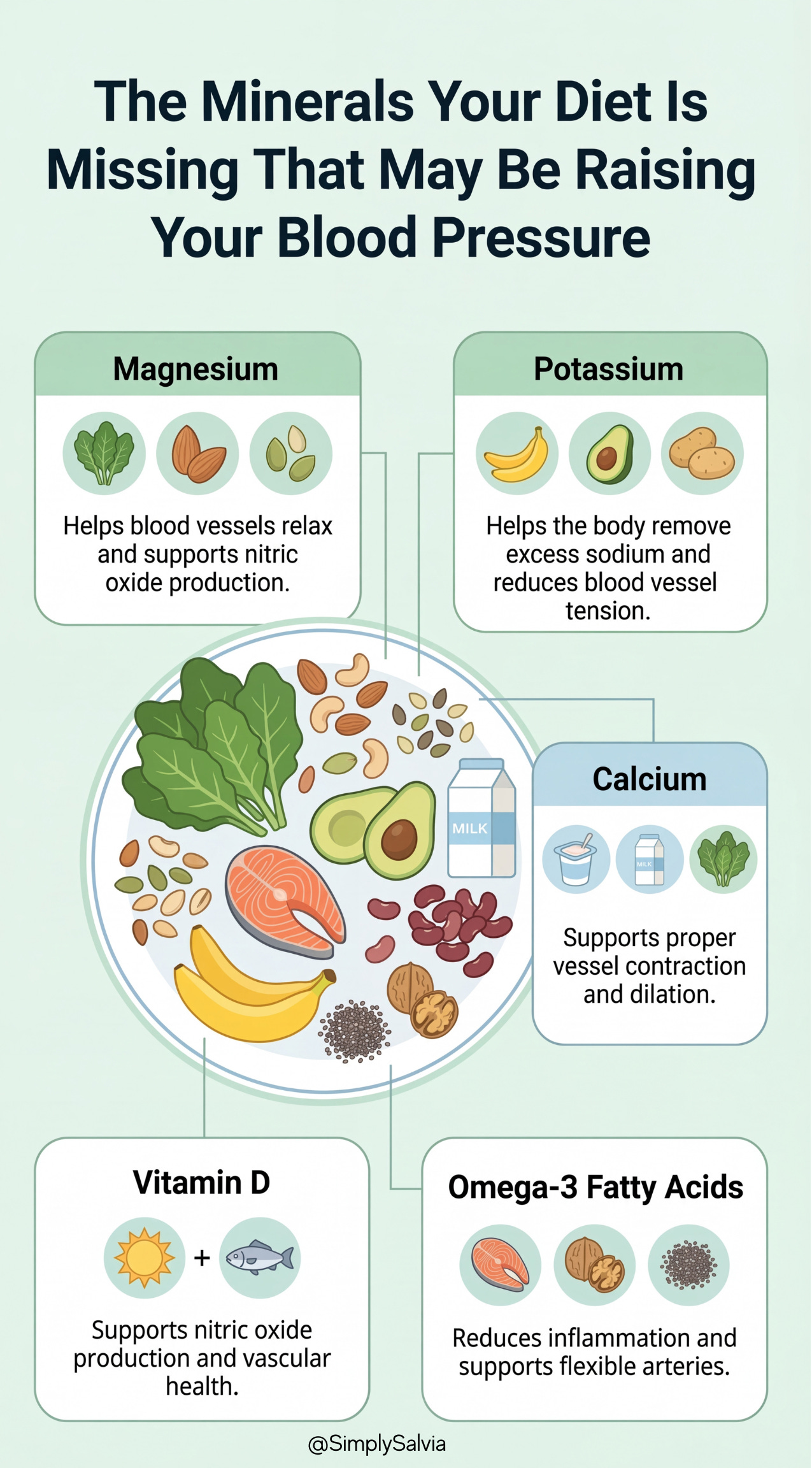
Modern diets can leave us deficient in key minerals and nutrients that help regulate blood pressure. One common example is magnesium.
Magnesium: The Mineral That Helps Your Vessels Relax
Magnesium is nature’s calcium channel blocker, it helps blood vessels relax. A lack of magnesium is linked to higher blood pressure, and increasing magnesium intake (through diet or supplements) can produce modest reductions in BP. Magnesium supports the production of nitric oxide (NO), a molecule that signals arteries to dilate (widen). Low magnesium, therefore, may impair this vasodilation pathway. It’s estimated that 500–1000 mg of magnesium daily could lower blood pressure by up to 5.6/2.8 mmHg in some people though results vary. Diets rich in green leafy vegetables, nuts, seeds, and whole grains provide magnesium that many processed-food diets lack.
Potassium: The Quiet Counterbalance to Sodium
Potassium works hand in hand with magnesium. Potassium helps the body excrete sodium and relax blood vessel walls. Diets low in potassium and high in sodium are a recipe for hypertension. Conversely, increasing potassium while reducing excess sodium is strongly proven to lower blood pressure. High potassium foods include fruits (like bananas, oranges), vegetables (potatoes, avocados, spinach), beans, and dairy. Sodium, of course, is a major culprit as high salt intake causes water retention and raises blood volume, increasing pressure. Many people consume far above the recommended <2.3 grams of sodium per day. Balancing sodium and potassium is critical: potassium helps offset sodium’s pressure raising effect.
Calcium & Vessel Tension: The Mineral You’re Probably Undereating
Calcium is another player. While the evidence is mixed, some studies suggest that inadequate calcium intake may contribute to high blood pressure. Calcium is involved in blood vessel contraction and dilation. Low calcium might trigger the body to retain more sodium or cause arterial constriction. Diets following the DASH plan (rich in low-fat dairy) have shown blood pressure improvements, hinting that sufficient calcium (along with magnesium and potassium) is beneficial.
Vitamin D: The Hormone-Like Nutrient Your Arteries Depend On
Vitamin D deficiency has been linked to hypertension as well. Vitamin D isn’t just for bones. It also interacts with blood vessels and the immune system. Low vitamin D levels are associated with arterial stiffness and endothelial dysfunction. One reason is that vitamin D helps stimulate nitric oxide production for vessel relaxation. In lab studies, adding vitamin D increased nitric oxide (the vessel-widening compound) and reduced inflammatory substances that damage vessels. Insufficient vitamin D may therefore reduce nitric oxide availability, contributing to higher vascular tone. Observational research shows people with deficient vitamin D tend to have higher rates of hypertension and are at greater risk of stroke. Getting safe sun exposure or supplements to reach adequate vitamin D levels (and thus support healthy blood vessels) may be helpful if one is deficient.
Omega-3s: The Anti-Inflammatory Fat Your Heart Loves
Lastly, a deficiency in omega-3 fatty acids (the heart healthy fats found in fish, flaxseed, etc.) may remove a natural protection against high blood pressure. Omega-3s (like EPA and DHA) have anti-inflammatory effects and help the endothelium (vessel lining) function well. Studies show that consuming about 2–3 grams per day of omega-3s can modestly reduce blood pressure. One analysis found around 4.5 mmHg drop in systolic BP for people with hypertension taking 3g of omega-3 daily. If someone’s diet is very low in omega-3 (and high in pro-inflammatory fats), they might miss out on these blood pressure lowering benefits. Omega-3s help vessels stay flexible and may stimulate nitric oxide, so a deficiency could tilt the body toward higher pressure. Eating fatty fish (like salmon, tuna) or plant sources of omega-3 (chia seeds, walnuts) regularly is a natural way to support healthy blood pressure.
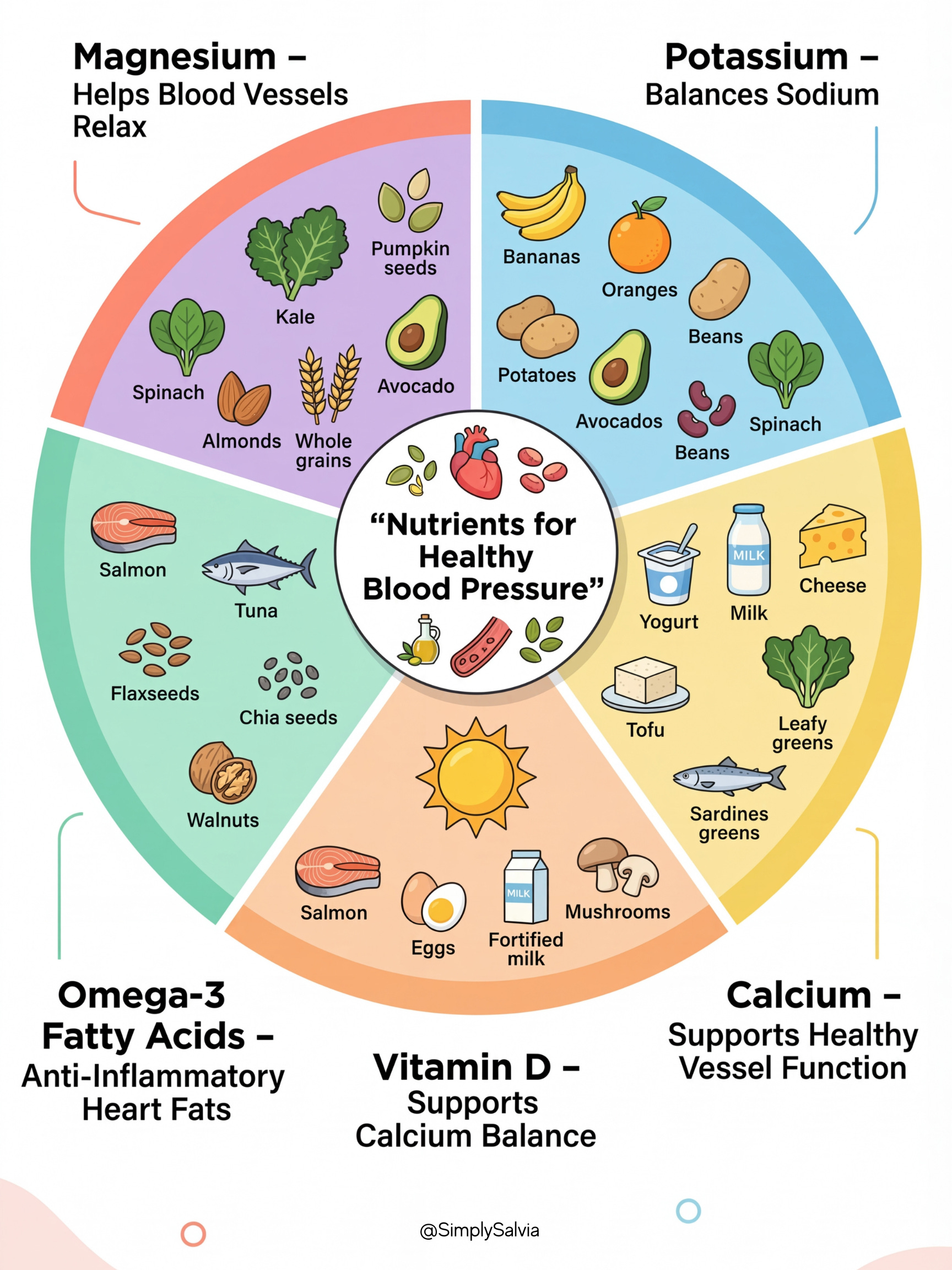
In summary, nutrient imbalances can contribute to hypertension. Modern diets high in processed foods often lack magnesium and potassium while overloading sodium creating a perfect storm for raising blood pressure. Ensuring adequate magnesium, potassium, calcium, vitamin D, and omega-3s through a balanced diet or supplements (if needed) can improve vascular health and complement blood pressure management. Later, I’ll discuss specific foods and supplements to boost these nutrients naturally.
4. You Can Feel Completely Fine and Still Have Dangerously High Blood Pressure
One of the most important things to understand about hypertension: it is almost entirely asymptomatic. You can feel perfectly fine while high blood pressure is quietly damaging your body. That’s why routine screening is so important. In most people, hypertension is asymptomatic (“silent”) hence the nickname “silent killer.” In fact, many patients only discover it during a doctor’s visit or through home monitoring, not because they felt anything wrong.
That said, extremely high blood pressure (or a sudden spike) can sometimes produce symptoms. Possible warning signs include:

However, these symptoms are not reliable indicators as they typically occur only in severe cases or hypertensive crises. For example, a hypertensive crisis (BP >180/120) may present with a severe headache, anxiety, nosebleed, and shortness of breath, and is a medical emergency. But someone with moderate hypertension (say 160/100) might have no clue.
It’s a common myth that high blood pressure always causes noticeable symptoms like frequent headaches or nosebleeds. In reality, if such symptoms occur, it’s usually because blood pressure has reached dangerously high levels over time. For instance, nosebleeds and headaches can happen, but by then BP may be crisis-level and organ damage could be underway. As one doctor put it: when symptoms do occur, high blood pressure may have already reached life-threatening levels.
Therefore, do not wait for symptoms to gauge your blood pressure status. The absence of symptoms is not a sign that all is well. Millions of people walking around with 140/90 or 160/100 feel normal. The first symptom of hypertension could tragically be a heart attack or stroke. That’s why hypertension is often discovered when patients present with complications rather than complaints of blood pressure itself.
This is especially relevant for the 15–35 age group, where there’s a cultural assumption that high blood pressure is an older person’s condition. The statistics don’t support that anymore.
In summary, often no symptoms – which means the only way to know your blood pressure is to measure it. Home blood pressure monitors and periodic checks at the clinic are invaluable. Be aware of subtle clues too: some hypertensive individuals report occasional flushed face, pounding in the ears or chest, or slight visual disturbances when BP is high. But these are inconsistent. Treat any severe acute symptoms (like intense headache + high BP reading, chest pain, neurological changes) as an emergency. Otherwise, assume hypertension is silent and stay vigilant with monitoring.
5. What Happens at the Doctor and What Those Numbers Actually Mean
Diagnosing hypertension is straightforward: it’s based on blood pressure measurements. Typically, if your BP is high on at least two separate days/visits, you may be diagnosed with hypertension. Doctors measure with a cuff and stethoscope or digital monitor. It’s important that the reading is done under standardized conditions; sitting quietly for 5 minutes, arm at heart level, no caffeine or smoking 30 minutes prior, to get an accurate baseline reading.
Understanding the two numbers is key: systolic (top number) is the pressure when the heart contracts, and diastolic (bottom number) is the pressure when the heart relaxes. Both are measured in mmHg (millimeters of mercury). A reading consistently ≥130/80 (per current American guidelines) or ≥140/90 (per older and global standards) indicates hypertension.
Sometimes, blood pressure readings in a medical office are higher than normal due to anxiety this is known as “white coat hypertension.” The nerves of being in a doctor’s office can spike the pressure temporarily. White coat hypertension is not benign: it occurs in an estimated 10–30% of patients and can be a precursor to sustained hypertension. To sort this out, doctors may use home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM). With ABPM, you wear a portable device that takes BP readings throughout your normal day and night. This provides a true picture of your typical blood pressure. If your office readings are high but home/ABPM readings are normal, you likely have white coat hypertension. Current guidelines don’t recommend drug treatment for isolated white coat hypertension if ambulatory readings are normal, but such patients should be monitored closely as many will develop true hypertension over time.
Conversely, some people have “masked hypertension,” where readings are normal at the doctor’s but high at home perhaps due to stress or lifestyle factors outside the clinic. Up to 1 in 3 adults with apparently normal office BPs may have masked hypertension identified by home monitoring. That’s why home blood pressure cuffs are so useful they can reveal if your pressure creeps up during daily life.
Ambulatory monitoring is especially helpful to confirm a diagnosis and check for patterns: for example, whether your BP dips at night (it should normally drop about 10-15% during sleep; if not, that can signal higher risk). It also can capture morning surges or episodes of very high BP that might be missed in single office checks.
In practice, a diagnosis is made after repeated measurements. A doctor might ask you to record your BP at home twice a day for a week. If the average of those readings is elevated, that clinches the diagnosis. They may also do basic tests (blood tests for kidney function, etc.) to see if there’s any secondary cause or damage.
It’s worth noting that on any given day, blood pressure fluctuates. Stress, exercise, even talking can raise it transiently. That’s why a single high reading isn’t enough to diagnose hypertension, it must be persistent. “Persistent” is usually defined as two or more properly measured readings ≥130/80 or ≥140/90 on different days. The threshold might differ slightly by organization, but the process is similar.
In summary, hypertension is diagnosed by measuring it – no fancy scans or symptoms needed, just a blood pressure cuff. Ensure readings are accurate and representative of your usual levels. If you suspect white coat effect, discuss home or ambulatory monitoring with your provider.
6. Normal, Elevated, Stage 1, Stage 2: Where Do Your Numbers Actually Fall?
Health professionals classify blood pressure into categories to better guide treatment. According to the American College of Cardiology/American Heart Association (ACC/AHA) 2017 guidelines (widely used in the U.S.), the stages are:
These categories highlight that both numbers matter. For instance, 135/95 is stage 2 because the diastolic of 95 is in stage 2 range, even though systolic is 135. On the flip side, 145/78 is stage 2 (systolic in stage 2) despite a normal diastolic.
It’s also notable that the ACC/AHA thresholds are a bit more aggressive than older schemes. Organizations like WHO or the International Society of Hypertension often consider 140/90 as the cutoff for hypertension. The ACC/AHA introduced the 130/80 definition to encourage earlier intervention, as evidence showed cardiovascular risk begins rising at those slightly lower levels. Under these guidelines, an “Elevated” BP (120-129/<80) is essentially pre-hypertension, a critical window for lifestyle changes to prevent progression.
To put it simply:
<120/80: great, maintain healthy habits.
120-129/less than 80: not yet hypertension, but higher than ideal so take action (diet, exercise) to prevent further rise.
130-139/80-89: Stage 1 – officially high BP. Depending on your risk factors, lifestyle changes and maybe medication might be recommended.
≥140/90: Stage 2 – clearly high, likely requiring medication in addition to lifestyle changes.
Less than 180/120: Crisis – requires immediate medical attention, especially if symptomatic (e.g. severe headache, vision changes, shortness of breath, etc.).
Understanding your category helps in gauging urgency. For instance, someone with 128/78 (elevated) should take steps to bring it down, even though it’s not “hypertension” yet. Meanwhile, someone at 145/95 (stage 2) should work closely with a doctor on a treatment plan to avoid serious complications. These stages provide a roadmap for both patients and providers to stratify risk and act accordingly.
Section 1 was the foundation.
You now know what the numbers mean, why your body drives blood pressure up and keeps it there, which nutritional gaps are quietly making it worse, and maybe most importantly — why you can feel completely fine while something serious is accumulating. That last part tends to stay with people.
But here’s where it gets more complicated. And more specific to you.
Because the story of blood pressure in women isn’t the same as the general story. The pill can raise it and most women on hormonal contraception are never told to monitor theirs. Your thyroid, your kidneys, a hormonal imbalance you might not know about yet — any of these can be the actual driver, which means the standard lifestyle advice will never be enough on its own. The oestrogen that’s been quietly protecting your cardiovascular system since puberty doesn’t stay forever. And then there’s pregnancy, where elevated blood pressure isn’t just a symptom to manage, but a warning signal with implications that follow you for decades.
Part 2 is where the research gets women-specific. And where the practical part starts.
In Part 2:
Section 2 covers what’s actually behind high blood pressure in women; the pill, the thyroid, the kidneys, the hormonal conditions that often go undiagnosed for years and what happens when oestrogen stops protecting you at menopause.
Section 3 is the evidence on what actually lowers blood pressure. Not the “cut salt and relax” version. The DASH diet versus Mediterranean eating, what the research says about hibiscus tea and magnesium and garlic, a full week of meals that are designed around blood pressure and actually look good, and the specific breathing practice that clinical studies show produces measurable reductions in just five minutes a day.
Section 4 covers the numbers that mean see a doctor right now, how every class of blood pressure medication actually works and why your doctor chose it, and, the section most women never get access to — what gestational hypertension and preeclampsia actually are, why a history of either doubles your long-term cardiovascular risk, and what to do with that information after pregnancy ends.
The 24-year-old from the beginning of this post? She came back for Part 2.
Upgrade to read Part 2 →