

Short Dive: Why You Get That Same Painful Breakout On Your Chin Every Month — And How to Actually Stop It (Part 1)
The breakouts on your lower face are not the same as the ones on your forehead. They have a different cause, a different biology, and they need a completely different approach.

There’s a specific kind of frustration that comes with jawline acne.
It’s not the frustration of a random pimple before an event. It’s the frustration of breakouts that follow a pattern you can almost set a calendar to — the same spot, the same week every month, the same deep, painful bump that takes two weeks to surface, peaks badly, and leaves a mark for another month after. You’ve done everything. Changed your cleanser. Cut out dairy. Tried benzoyl peroxide. Bought the spot treatment everyone on TikTok swears by. Simplified your routine. Complicated your routine.
And the jawline keeps breaking out.

Not because you’re doing something wrong. Because you’re treating a hormonal problem with skincare solutions and that gap is why nothing sticks.
Here’s what most acne content doesn’t say clearly enough: jawline and chin breakouts are biologically different from the ones on your forehead or nose. Research consistently shows that lower-face acne in adult women is predominantly hormonal in pattern, driven by androgens that overstimulate oil glands in that specific region, producing the deep, cystic, under-the-skin bumps that don’t respond to standard pore-clearing treatments because they didn’t form in the pore to begin with. They formed underneath it.
This is why the same salicylic acid face wash that cleared your T-zone in 2019 is doing nothing for your jaw in 2025. Different mechanism. Different depth. Different origin.
And here’s where it gets more specific: the cluster of acne along the lower cheeks, jawline, and chin — that exact geography, maps almost precisely onto where androgens do their work. Androgens like testosterone and DHT drive sebum production disproportionately in this region, which is why women with hormonal fluctuations, around their period, under chronic stress, coming off the pill, or with conditions like PCOS tend to break out in the same zone, in the same way, on a loop.
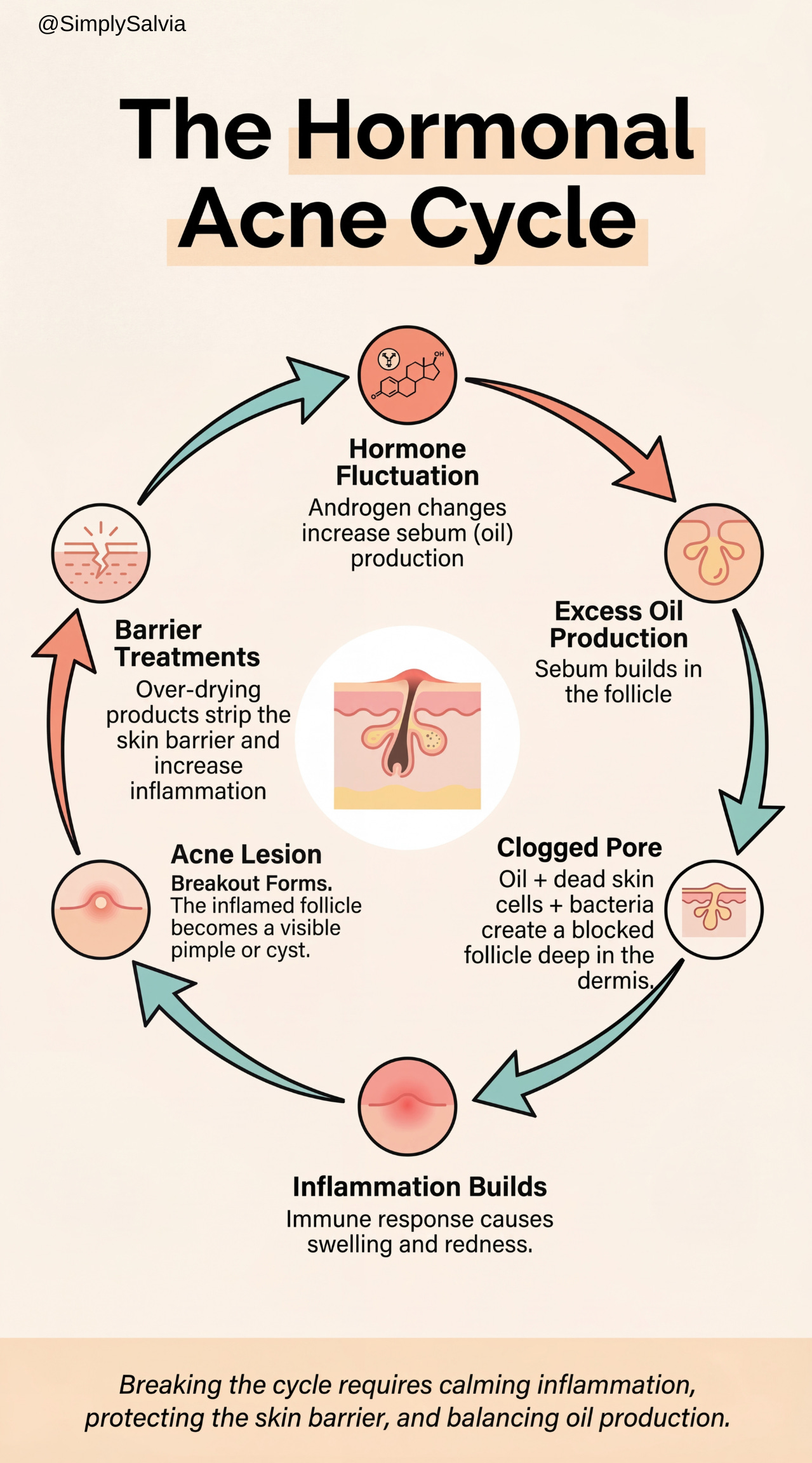
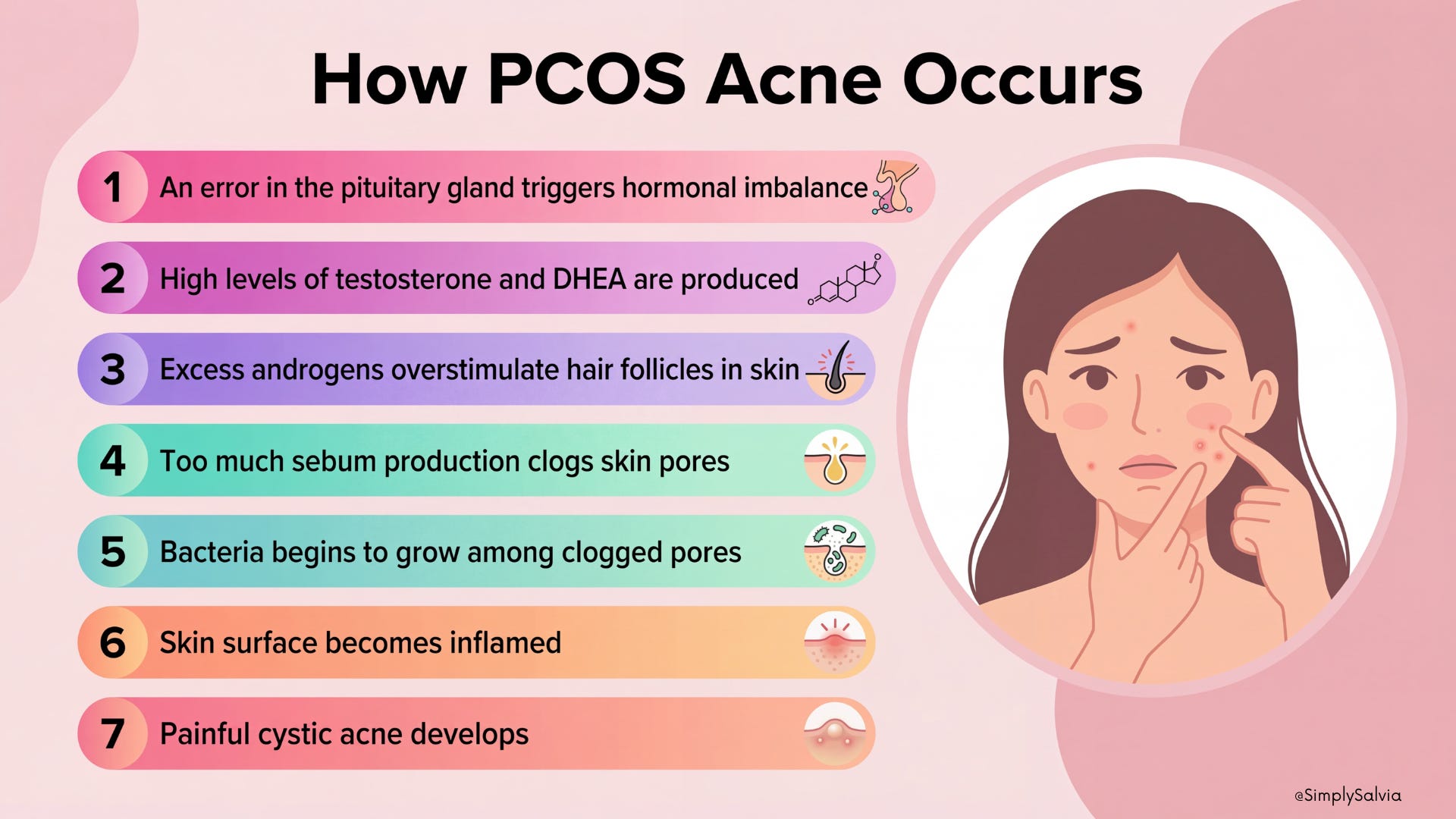
The loop looks like this. Hormone fluctuation triggers excess oil. Excess oil combined with dead skin cells and the right bacteria creates a clogged follicle deep in the dermis. Inflammation builds. The bump forms. Harsh treatments strip the skin barrier trying to dry it out, which triggers more inflammation, which makes the hormonal response worse. More breakouts. More product. More stripping. More breakouts.
Most women stay in this loop for years. Not because they’re not trying but because nobody explained the loop.
I started researching this because I couldn’t find one place that connected all of it. The hormones. The gut. The specific ingredients in products that are making it worse without anyone flagging them. The dietary patterns that show up in dermatology research as genuinely linked to sebum and inflammation. The herbs and supplements with actual clinical evidence behind them versus the ones that are just trending.
What I found is that the science on hormonal acne has moved significantly in the last decade. Research into the gut-skin axis shows that the bacteria in your digestive system influence the hormonal pathways that drive sebum production, which is why the same antibiotics that clear skin temporarily often stop working, and why dietary patterns affect breakouts in ways that aren’t just about “eating clean.” Studies on insulin and IGF-1 show that blood sugar instability is one of the most direct dietary drivers of hormonal acne — more directly than dairy, more directly than chocolate, more directly than most of the things women get told to cut.
And there are conditions; PCOS, thyroid imbalances, adrenal dysfunction, where the jawline acne is not a skincare issue at all. It’s a symptom. And no serum is going to fix a symptom when the underlying condition is still running in the background.
The question isn’t what should I put on my jawline. It’s what is my jawline trying to tell me.
This Short Dive covers:
The jawline is not random. It’s specific. And specific problems have specific answers — if you know where to look.
PS: We also have a subscriber-only group chat where members discuss the deep dives, share their sleep journeys, and ask me questions directly. See you there.
Disclaimer: The information and opinions expressed above are current as of the date of this post and are subject to change without notice. Materials referenced above are provided for educational and informational purposes only. None of the above constitutes medical advice, a diagnosis, a treatment recommendation, or a substitute for consultation with a qualified healthcare professional. Always seek the guidance of your doctor or another qualified health provider with any questions you may have regarding a medical condition or sleep disorder.
Short Dive below ↓
CHAPTER 1: What Is Jawline Acne and Why Is It So Stubborn?
Spoiler: it starts way deeper than your pores.
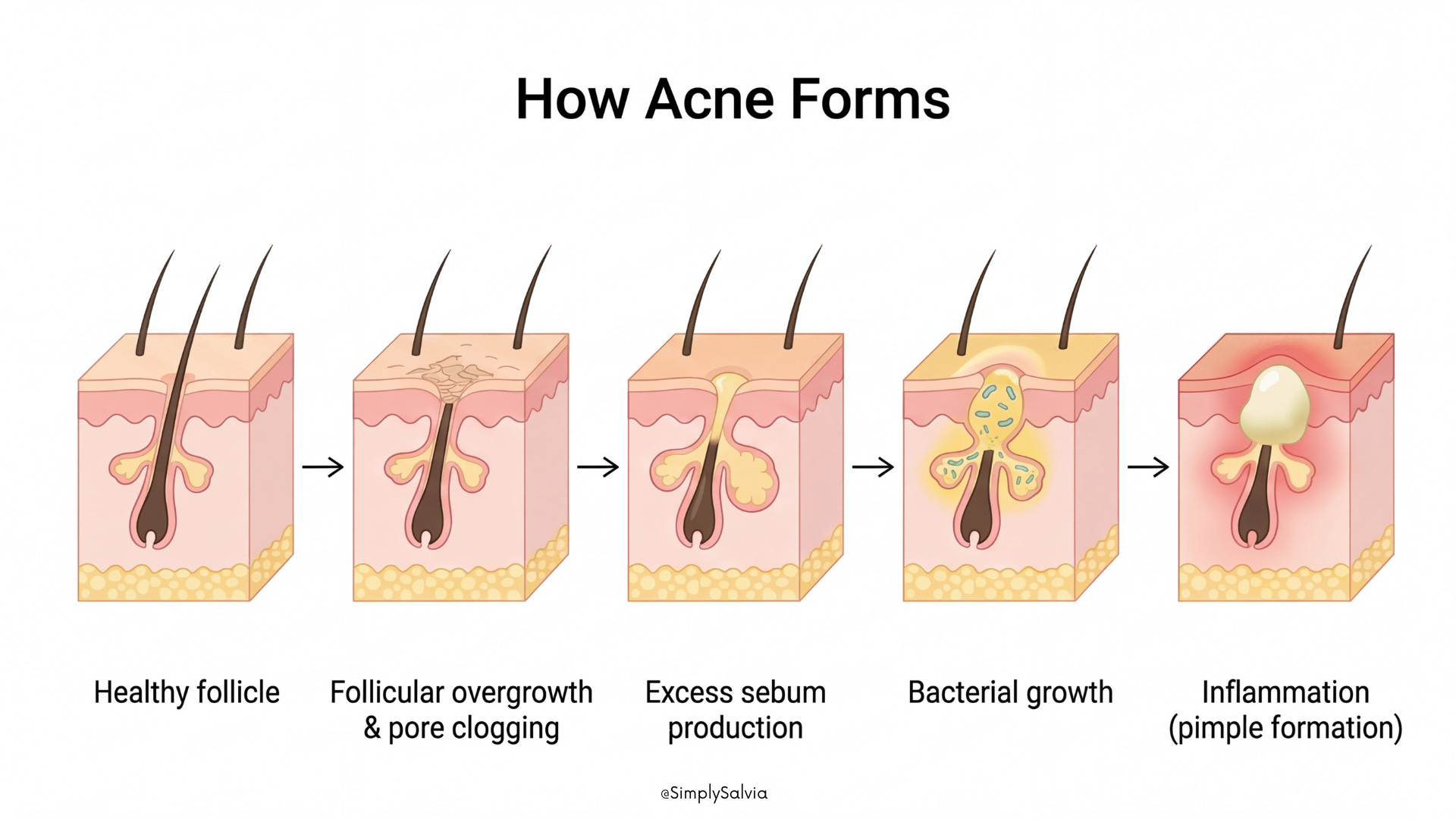
To understand why jawline acne happens, it helps to first understand how acne forms in general.
Every pimple begins in something called the pilosebaceous unit, which is simply a hair follicle and the oil gland attached to it. These tiny structures exist all over your skin and are responsible for producing sebum, the natural oil that keeps your skin soft and protected.
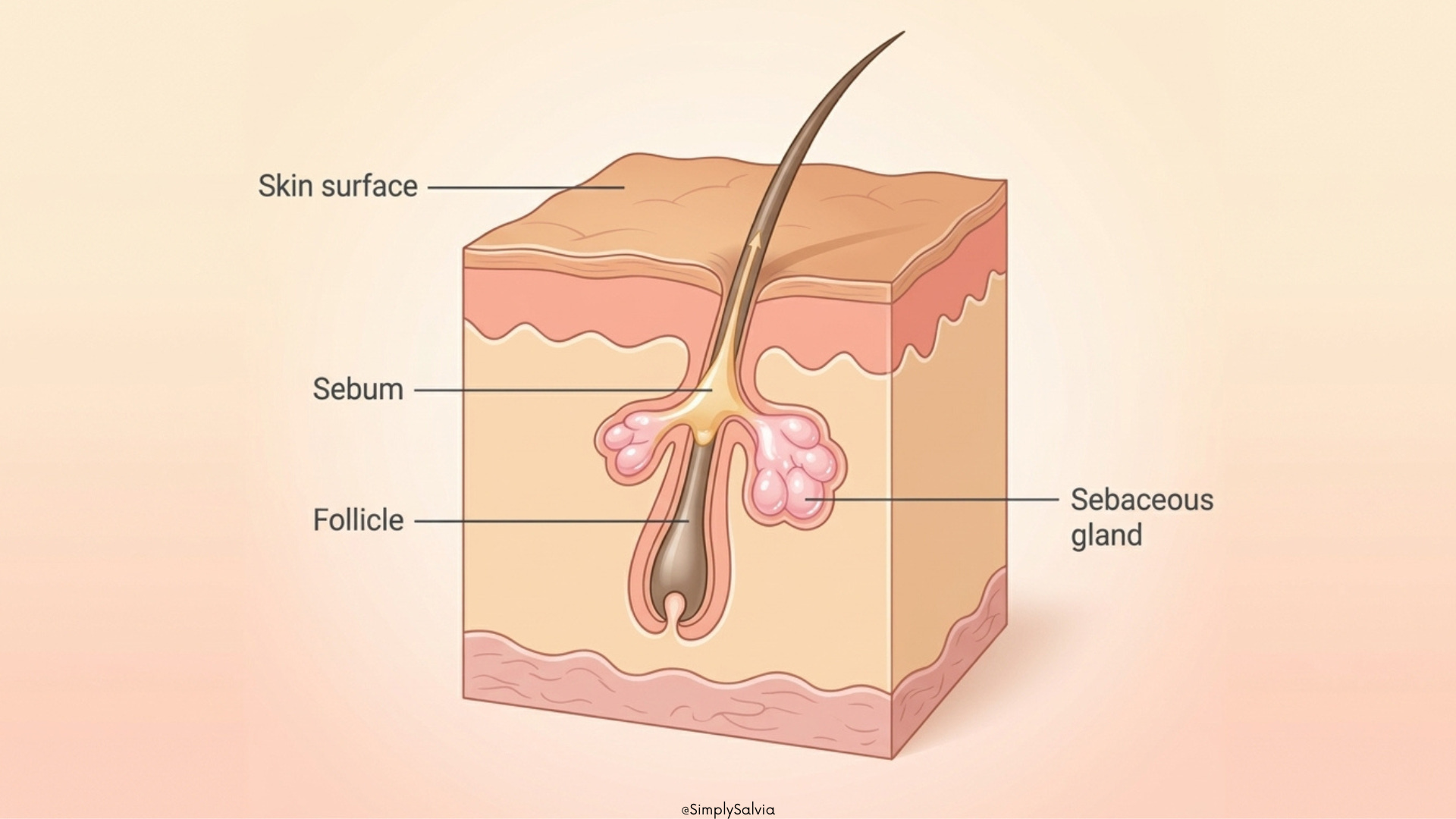
Under normal circumstances, this oil travels smoothly up through the pore and spreads across the skin’s surface. But acne begins when that system gets disrupted.
Hormones are often the first trigger. During times of hormonal change like puberty, menstrual cycles, or periods of stress, the sebaceous glands can start producing more oil than the pore can handle.
At the same time, dead skin cells that would normally shed from the surface don’t fall away properly. Instead, they stick together inside the pore, especially when there’s extra oil present. The combination of oil and dead skin cells creates a plug, which blocks the pore. This is the earliest stage of acne, known as a comedo (what we recognize as a blackhead or whitehead).
Once a pore is clogged, it becomes the perfect environment for bacteria to thrive. One of the main bacteria involved in acne is Cutibacterium acnes (formerly called Propionibacterium acnes). These bacteria naturally live on the skin, but inside a blocked pore they can multiply quickly.
Your immune system notices this buildup and responds by triggering inflammation. That’s why pimples become red, swollen, and sometimes painful.
So in simple terms, acne develops when four things happen together:
• excess oil production
• dead skin cells clogging the pore
• bacterial growth inside the blockage
• inflammation from the immune response

Genetics also plays a role in this process. Some people naturally produce more oil, while others have pores that clog more easily. This means certain individuals are simply more prone to acne than others, even when they follow the same skincare routine.
Why Jawline Acne Feels Different
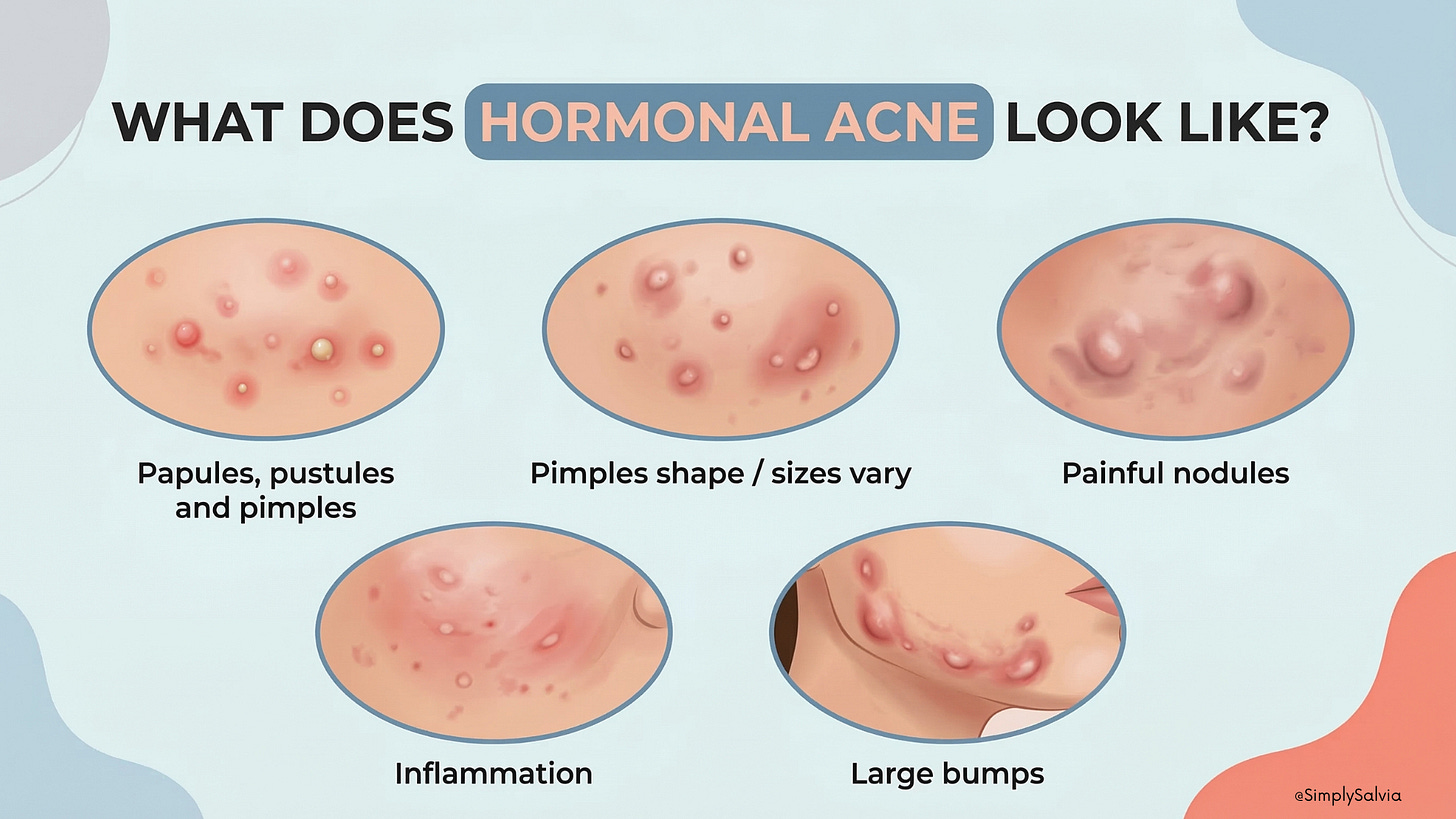
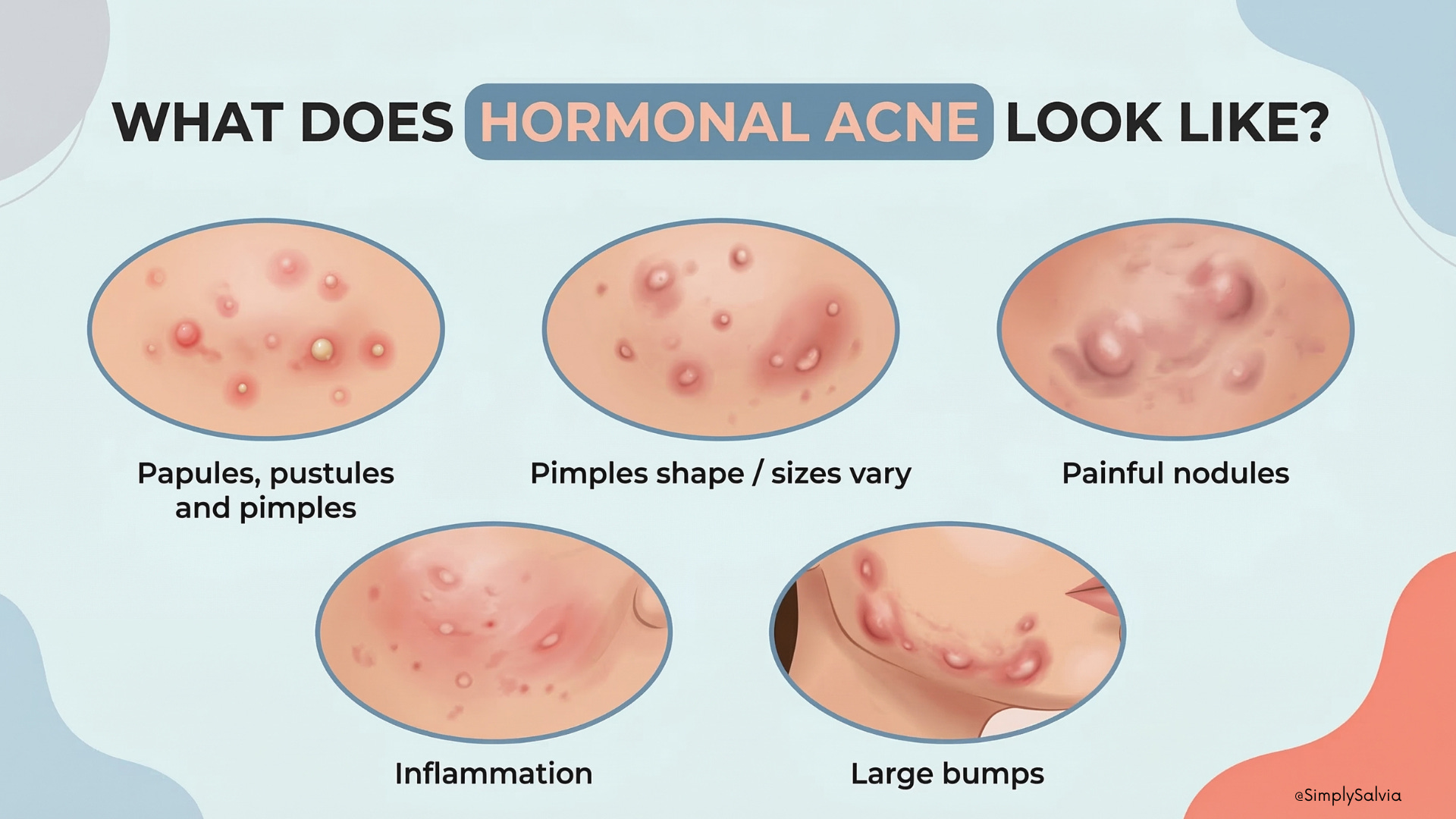
Jawline acne follows the same basic process as any other type of acne — clogged pores, excess oil, bacteria, and inflammation. But acne in this area tends to behave a little differently. What makes jawline acne unique is that it’s often deeper and more cystic than the breakouts you might get on your forehead or nose. Dermatologists frequently see this pattern in adult women, where breakouts appear along the lower face, jawline, and chin. This type is often referred to as hormonal acne. Instead of small surface whiteheads, these breakouts tend to form deep nodules or cysts beneath the skin. This happens when the blockage and inflammation occur deeper inside the pore, leading to a larger, more swollen lump. These bumps can feel firm, tender, and painful, and they often don’t develop a visible “head” like typical pimples do. Instead, they sit under the skin and can linger for days or even weeks before slowly resolving.
Because these breakouts are deeper and more inflamed, they also carry a higher risk of leaving marks or scars, especially if they’re picked or squeezed. That’s why jawline acne often requires a slightly different approach compared to more superficial breakouts.
Another hallmark: jawline and chin breakouts often correlate with hormonal swings for example, flaring up right before a period or during times of stress when cortisol rises. Hormones can stimulate the oil glands in the skin, causing them to produce more sebum than usual. This extra oil increases the chance of pores becoming clogged, which is why hormonal shifts often trigger deeper, cystic breakouts.
Dermatologists have observed that when acne consistently appears along the chin and jawline, it often follows a hormonal pattern. In fact this pattern is so recognized that persistent jawline acne in women is considered a red flag for possible hormonal imbalance like polycystic ovary syndrome (PCOS).
Why does jawline acne matter so much?
Beyond the cosmetic frustration, it’s a sign our body may be trying to tell us something. Because it’s often hormonally driven, jawline acne can be a window into internal issues for instance, imbalanced androgen levels or stress-related endocrine shifts. And since these cystic pimples can scar, treating them early and holistically is key to preserving skin texture. Finally, jawline acne often doesn’t respond as well to typical over the counter remedies (like benzoyl peroxide or salicylic acid) that might clear up milder acne. Cysts are more stubborn, so a different approach – one that addresses root causes (like hormones, diet, and skin care habits) is needed. The rest of this short dive will delve into those root causes and arm you with a variety of natural, science-backed strategies to calm your skin.
In short: Jawline acne forms through the same clogging and inflammation process as any acne, but it tends to be deeper, more hormonal, and more prone to scarring, meaning we need to pay special attention to what’s happening inside our bodies, not just slap on topical spot-treatments.
CHAPTER 2: Why Is Your Jawline Full of Oil and Acne?
Jawline acne doesn’t have a single cause it’s usually multifactorial, meaning several influences pile up to create the perfect storm for breakouts. Let’s break down the major categories of causes:
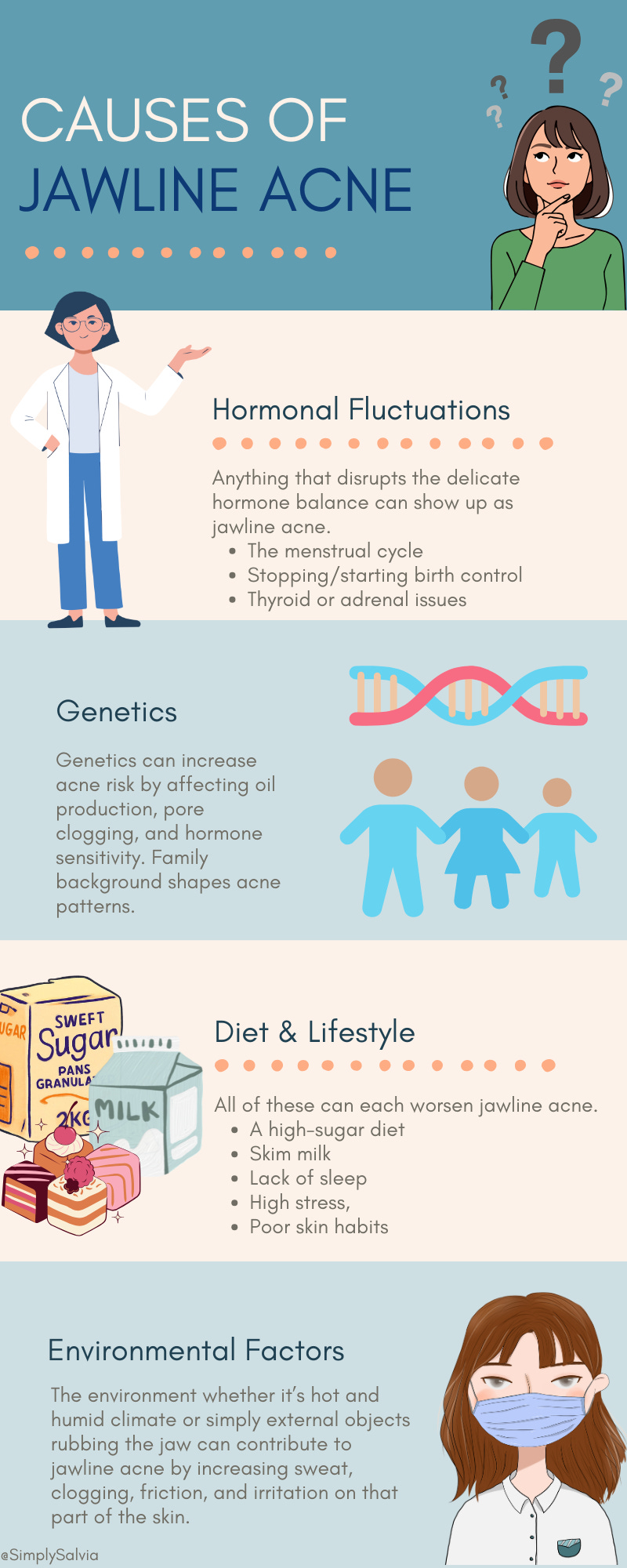
Hormonal Fluctuations
Hormones are often the number one culprit in jawline breakouts. Androgens (like testosterone) stimulate sebaceous glands to produce more oil. Women experience natural androgen surges before menstruation, which can explain those monthly chin pimples. Events like pregnancy or menopause also involve big hormonal swings that can trigger jawline acne. For example, during pregnancy some women’s skin clears due to high estrogen, while others breakout if androgen or progesterone levels spike. A common condition linked to jawline cysts is Polycystic Ovary Syndrome (PCOS) which is characterized by excess androgens. Women with PCOS often notice persistent, deep acne along the lower face, sometimes accompanied by other signs like irregular periods or increased facial hair. Even stress hormones play a role: chronic stress elevates cortisol, which in turn can increase skin’s oil production and inflammation. (Ever notice how a stressful week leads to a jaw breakout?).
Genetics
Our genes set the baseline for how reactive our skin is. If you come from a family where “bad acne” was common, you may have inherited skin that naturally produces more oil or sheds cells in a way that clogs pores easily. Family history is a known risk factor for severe acne. Genetics can also determine how sensitive your skin’s sebaceous glands are to hormones. Some people’s glands overreact to even normal levels of androgens – think of it like a genetic sensitivity leading to oilier skin and more clogged pores. There’s also research suggesting certain ethnic backgrounds may have different acne patterns or severity, potentially due to genetic differences in inflammation and skin structure. While you can’t change your DNA, knowing genetics are at play reminds us that acne is not your fault or due to “dirty skin” often it’s in your blueprint. The upside: even genetically oily or acne-prone skin can be managed with the right routine and lifestyle (it just means you have to be a bit more diligent).
Diet & Lifestyle
What we eat and how we live can significantly affect our skin’s behavior. Let’s start with diet: High-glycemic foods (think sugary snacks, white bread, sweetened drinks) cause blood sugar spikes, which trigger insulin surges. High insulin can ramp up androgen activity and Insulin-like Growth Factor (IGF-1), leading to more sebum production and clogged pores. Studies have found that individuals who consume lots of high-glycemic-load foods tend to have worse acne, while low-glycemic diets (focused on whole grains, beans, veggies) can improve breakouts. Dairy especially skim milk has also been linked to acne in multiple studies. One large analysis found that people who drank skim milk regularly had a 44% higher risk of acne than those who didn’t. The theory is that dairy proteins and hormones can stimulate the skin’s oil glands or inflammation (though not everyone is equally sensitive). Aside from food, consider lifestyle factors: Sleep is huge. Poor sleep or erratic sleep schedules can throw off your hormonal balance (raising cortisol, disrupting melatonin and growth hormone) and impair skin healing. It’s been observed that many acne sufferers report worse breakouts when they’re chronically tired or pulling all-nighters. Stress ties in here too, high stress levels correlate with more severe acne, likely because of stress hormones and inflammatory chemicals; in one study, 60% of acne patients said their acne worsened during stressful periods. Additionally, how we care for our skin day to day matters. Inconsistent or harsh skincare routines can backfire. For example, over-washing your face or using strong soaps can strip natural oils and paradoxically trigger rebound oiliness (the skin producing even more sebum to compensate). On the other hand, not cleansing at all or sleeping in makeup can lead to pore congestion. It’s a fine balance. Finally, basic hygiene: things like not changing pillowcases frequently or constantly touching your jaw/chin during the day can introduce bacteria or dirt to the area, aggravating acne.
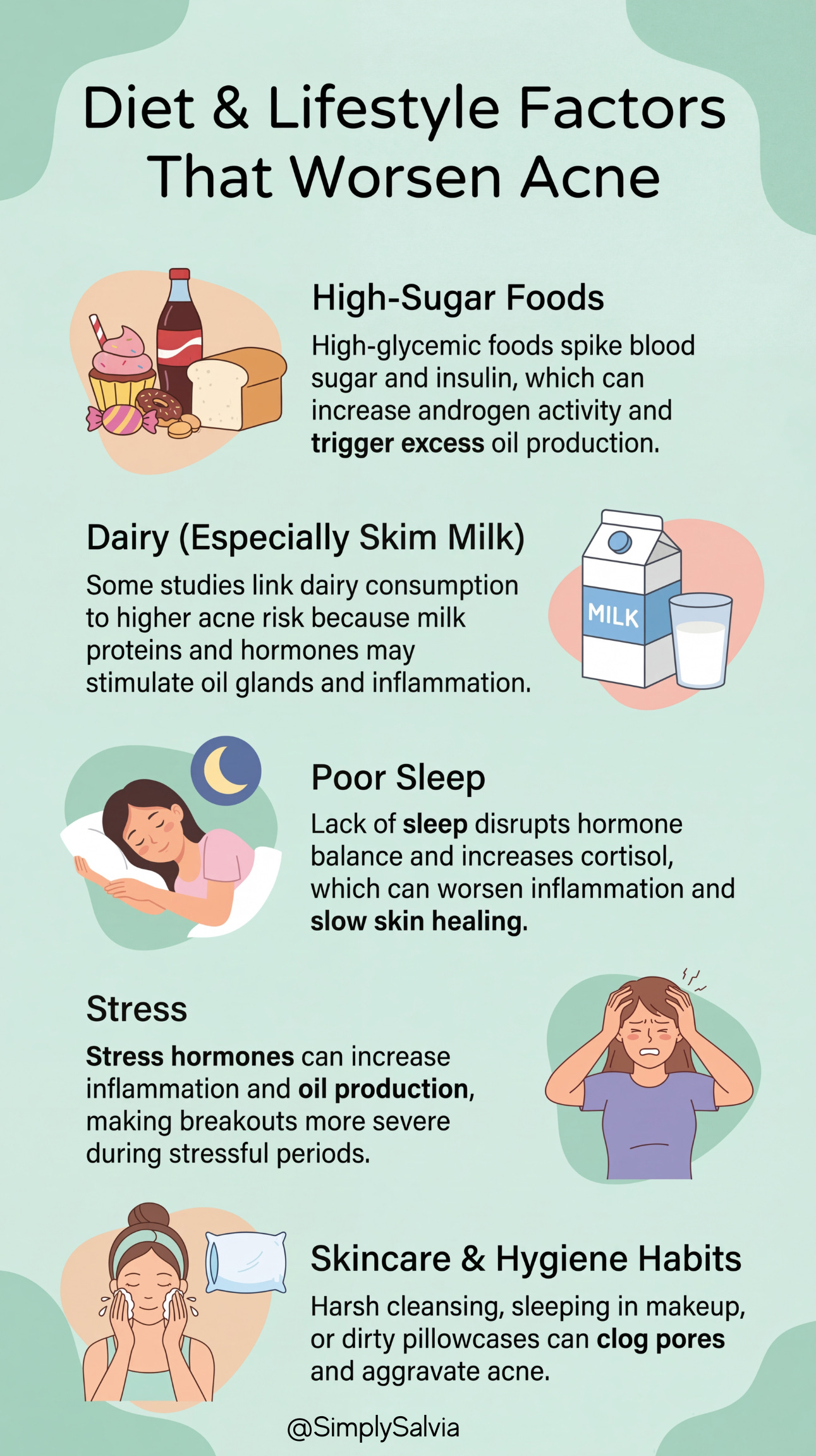
Summing up lifestyle: a high-sugar diet, skim milk, lack of sleep, high stress, and poor skin habits can each worsen jawline acne, but the good news is these are modifiable factors we can work on.
Environmental Factors
Sometimes the outside environment plays a role in jawline breakouts. Humidity and sweat can exacerbate acne because when the skin is moist and sweaty for prolonged periods, pores are more likely to get clogged. People in tropical or humid climates often report their acne gets worse in the summer, the term “summer acne” is even used. Sweat itself can irritate the skin if it’s sitting there mixed with dirt (especially under a mask or helmet strap against the jawline). This brings us to “maskne,” a nickname for acne mechanica; pimples caused by the rubbing and occlusion of wearing a face mask (common along the jaw and chin). The COVID-19 pandemic gave many people their first experience of jawline breakouts purely from that constant friction, trapped sweat, and bacteria under a mask.
Pollution is another factor: airborne pollutants (like particulate matter from car exhaust or smoke) can settle on the skin and generate free radicals that irritate pores. While research is ongoing, some studies suggest that people in urban, polluted areas have higher rates of acne, possibly because these microscopic particles can induce inflammation or oxidative stress in the skin. Then there’s the physical environment: if you’re frequently resting your hand on your jaw while sitting (transferring oils/bacteria from your hand) or if you have long hair that sweeps your jawline and introduces oils or hair product residue, these seemingly small things can trigger breakouts in that area. Even cosmetics or sunscreen on the jaw/neck that are not fully cleaned off can clog pores there (we often apply sunscreen down to the jaw but might rinse our faces quickly without reaching the jawline edges thoroughly). And let’s not forget sports gear or musical instruments; violin chinrests, football helmet straps, etc., can cause pressure and occlusion on the jaw area, again leading to acne.
CHAPTER 3: Could Something Bigger Be Going On?
Sometimes, persistent jawline acne is more than a standalone skin issue, it can be a sign of an underlying health condition that’s affecting your hormones or metabolism. Here are some conditions to consider especially if jawline cysts are severe and accompanied by other symptoms:
Polycystic Ovary Syndrome (PCOS)
This is one of the first things to evaluate for in women with stubborn jawline acne. PCOS is an endocrine disorder characterized by ovarian cysts, irregular menstrual cycles, and excess androgen hormones. That excess testosterone is a major acne trigger. Women with PCOS often have acne that flares on the lower third of the face i.e. jawline, chin, upper neck, and the pimples tend to be deep and inflamed. Other clues of PCOS include thinning scalp hair or increased facial/body hair, weight gain, and difficulty with ovulation. Essentially, PCOS-related acne is a direct result of hormonal imbalance, especially elevated androgens and often insulin resistance (many PCOS patients have high insulin levels which further drive androgens). If you suspect this, a doctor can run tests (for testosterone, DHEA, blood sugar, etc.). The good news is that treating PCOS (through diet, exercise, medications like metformin or hormonal therapy) often dramatically improves the skin as well.
General Hormonal Imbalance
Even outside of PCOS, other hormone issues can cause jawline breakouts. For instance, if your estrogen and progesterone are very low (as can happen in perimenopause or after stopping birth control pills), androgens can have more relative influence, leading to acne. Some women have naturally high androgen levels or heightened sensitivity in the skin to normal levels, a condition sometimes termed “hormonal acne” without a specific named syndrome. Additionally, postpartum (after giving birth) many women break out because during pregnancy their hormones protected the skin, and once those hormones drop, acne can rebound. In short, anything that tilts the balance in favor of androgens or against estrogen/progesterone can prompt jawline acne. If irregular periods, hair changes, or other systemic symptoms accompany your acne, a hormonal work-up might be warranted.
Adrenal Fatigue or HPA Axis Dysregulation
The term “adrenal fatigue” is used in integrative medicine to describe chronic stress overtaxing your adrenal glands (which produce cortisol and other stress hormones). While not a formally recognized medical diagnosis, the concept is that prolonged stress disrupts your HPA axis (hypothalamus-pituitary-adrenal axis), leading to cortisol spikes and crashes. Cortisol can aggravate acne by increasing inflammation and oil production. People experiencing this might notice they get acne flares during high stress and also feel symptoms like fatigue, insomnia, or anxiety. Chronic stress can also indirectly mess with other hormones (for example, it can steal resources from progesterone to produce more cortisol, potentially leading to relative estrogen dominance or androgen excess). So if you’re burning the candle at both ends and your jawline is flaring, your body might be saying it’s time to manage stress better. Techniques like mindfulness, better sleep (as mentioned, poor sleep can worsen cortisol imbalance), and adaptogenic herbs are often suggested to support the HPA axis. While “adrenal fatigue” isn’t a straightforward clinical condition, the underlying idea that stress hormones affect skin is absolutely valid and many dermatologists agree stress-related cortisol surges can trigger breakouts.
Hypothyroidism
An underactive thyroid (hypothyroidism) might not be the first thing you think of with acne as classic hypothyroid symptoms are dry skin, fatigue, weight gain. However, the body’s hormonal web is intricate. Thyroid hormone levels can influence the skin’s texture and the turnover of skin cells. Some reports suggest hypothyroidism can indirectly contribute to acne by causing a sort of sluggishness in the skin’s regeneration and possibly altering sex hormone levels (low thyroid function can lead to higher levels of thyroid-stimulating hormone and possibly increased prolactin, which might have minor androgen-raising effects). Moreover, hypothyroid individuals sometimes have imbalances in estrogen/progesterone (for women, thyroid and reproductive hormones often interact). There’s also a connection with insulin resistance at times. While evidence is mixed, one recent study found a higher prevalence of autoimmune thyroiditis (Hashimoto’s disease) in people with moderate to severe acne, suggesting a link between thyroid dysfunction and acne severity. In that study, hypothyroidism and insulin resistance were both associated with more severe, stubborn acne. The takeaway: if you have other signs of hypothyroid (cold intolerance, heavy fatigue, hair thinning, irregular cycles) along with jawline acne, consider checking your thyroid as treating an underactive thyroid might improve your skin indirectly.
Insulin Resistance & Metabolic Syndrome
I touched on diet’s role in acne; insulin resistance is the physiological state underlying issues like pre-diabetes and metabolic syndrome. When cells become resistant to insulin, the body compensates by pumping out more insulin. High insulin levels can spur the ovaries (and adrenal glands) to produce more androgens. This is why conditions like metabolic syndrome and PCOS often overlap as both involve insulin resistance and come with acne as a symptom. Research has shown that acne patients are more likely to have insulin resistance, and conversely, that those with insulin resistance often have more severe acne. Signs of insulin resistance include weight around the midsection, skin tags, acanthosis nigricans (dark velvety patches often on the neck or underarms), and sugar cravings or energy crashes. If your jawline acne coincides with these signs, addressing insulin resistance (through a low-glycemic diet, exercise, possibly medications like metformin) could significantly help. In one study, individuals with acne and insulin resistance who adopted a low-glycemic diet saw improvement in acne as their insulin sensitivity improved.
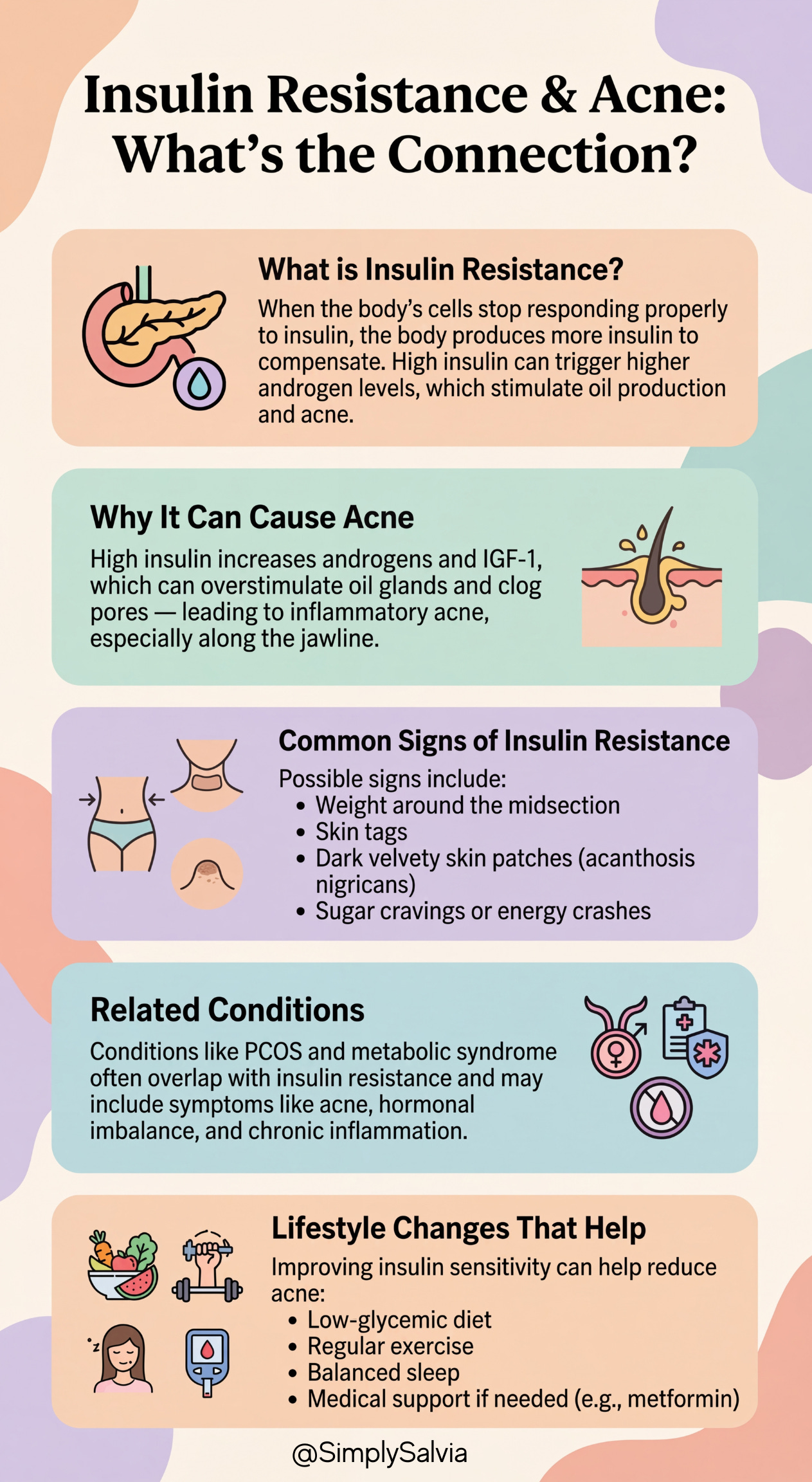
Metabolic syndrome (a cluster of high blood pressure, high blood sugar, abnormal cholesterol, and abdominal obesity) is another condition where chronic inflammation is present, this systemic inflammation can make the skin more prone to inflammatory acne as well. So yes, your jawline acne could be your body’s way of waving a flag about blood sugar and metabolism issues. The encouraging part is that these issues can often be turned around with lifestyle changes, benefiting your whole body and your skin.
Bottom line: If your jawline acne is persistent, severe, or accompanied by other symptoms like irregular periods or weight changes, it’s wise to consider underlying conditions. PCOS is a big one for women, but also check on thyroid function, stress hormone balance, and blood sugar/insulin status. Treating the root cause whether through medical or natural means can lead to much more effective and long-lasting clearing of the skin.
CHAPTER 4: Wait — What Kind of Acne Do You Actually Have?
Not all breakouts are the same. Knowing yours changes your approach.
Not all pimples are created equal! Understanding what type of acne you have can guide you to the right treatments. Jawline acne is often hormonal, but you might also experience other types. Let’s break down the common acne variants and how to tell them apart:
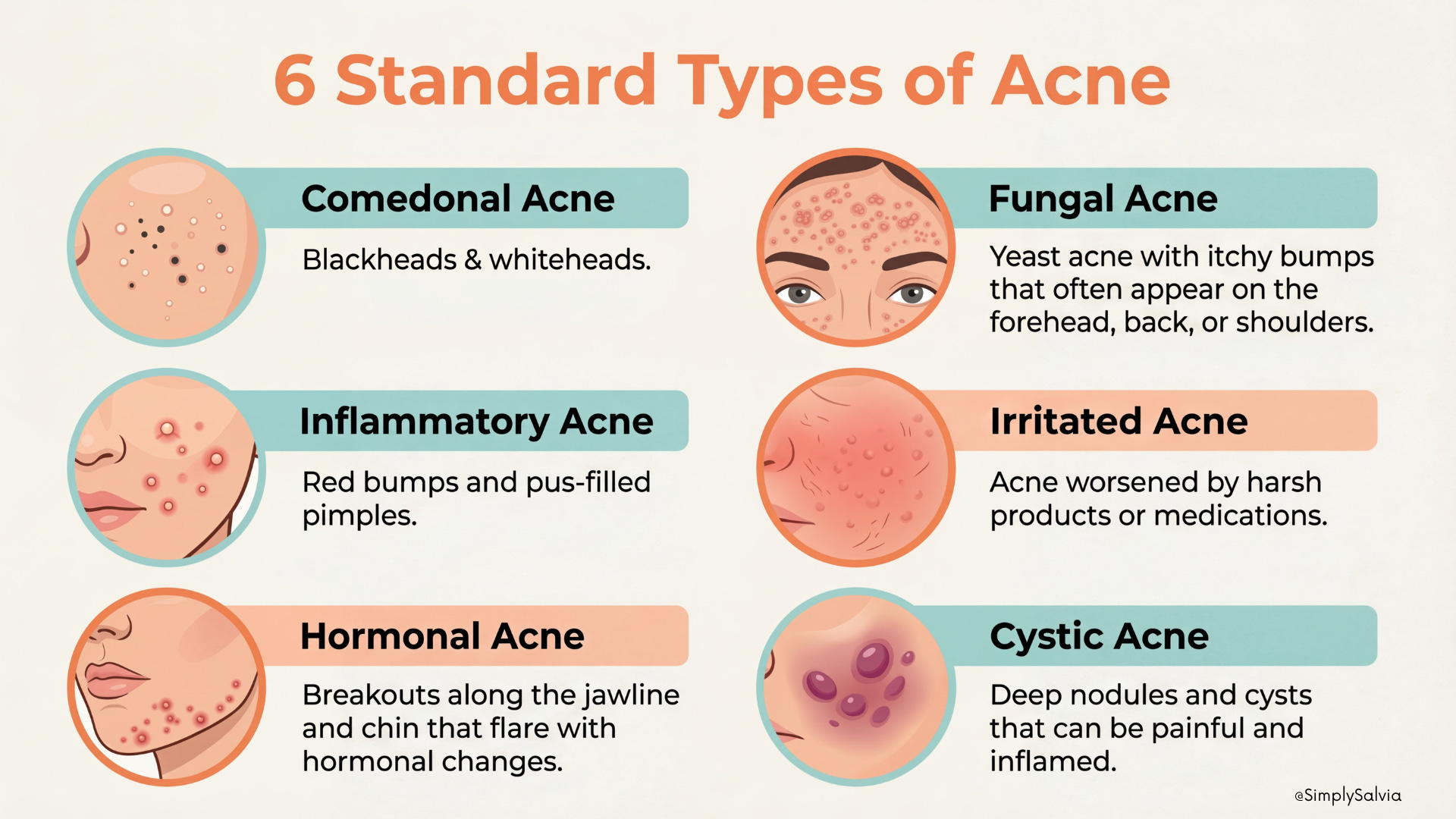
Hormonal Acne: Hormonal acne, refers to the pattern often seen in adult women – deep, cystic breakouts concentrated along the chin, jawline, and neck. Key features: lesions are often cysts or nodules (under the skin bumps that can be painful), rather than just surface pustules. They tend to flare cyclically, for women, typically pre-menstrual or during times of hormonal flux. You might notice they coincide with other signs of hormonal swings (mood changes, etc.). Hormonal acne can also affect men for instance, if testosterone levels are high or during certain life stages, but in women it’s very pronounced. If your acne is mostly along the jaw/chin and consists of those big, tender bumps that don’t come to a whitehead, it’s very likely hormonal in nature. Treating it often requires internal approaches (diet, stress management, hormonal therapies) in addition to topicals.
Bacterial/Inflammatory Acne: This refers to the classic acne vulgaris that many teens get, caused by the bacteria C. acnes and characterized by red, pus-filled pimples. These are the zits that start as clogged pores but then get invaded by bacteria and inflamed, turning into pustules (a pimple with a white or yellow center of pus) or papules (red bumps). They can occur anywhere on the face. If you’re seeing a lot of traditional “zits” the kind you might be tempted to pop because they have a visible white head then that’s inflammatory acne. Jawline areas can get these too, especially if bacteria from frequent touching or sweat is involved.
Bacterial acne lesions are usually smaller and more superficial than cysts. They also typically respond well to antibacterial treatments (like benzoyl peroxide or tea tree oil). One way to tell hormonal cysts from regular bacterial pimples is size & depth: cysts are larger, deeper, and rarely have “heads,” whereas bacterial pustules are more surface-level with obvious pus. However, inflammatory acne is a broad term that includes cysts too essentially any acne lesion that is red/swollen is inflammatory. It’s just that some are primarily driven by bacteria, while others (like cysts) are more tied to hormones and inflammation from within. The presence of many pustules and papules suggests a bacterial/inflammatory type predominance.
Comedonal Acne: These are the non-inflamed clogged pores: blackheads and whiteheads. Blackheads (open comedones) are pores clogged with oil and dead skin where the top has oxidized, turning it black or dark. Whiteheads (closed comedones) are similar clogs but with a layer of skin over the top, so they appear as small white or flesh-colored bumps. Comedonal acne tends to give the skin a rough, bumpy texture but without much redness. If you run your fingers over your jawline and feel many tiny bumps that aren’t red or sore, those could be closed comedones. These often result from things like using comedogenic (pore-clogging) skincare products or makeup, or not exfoliating enough so that dead cells build up. Comedonal acne is more common on the forehead and chin, but it can occur along the jaw especially if, say, you use a heavy cosmetic along the jawline or a not so clean phone held against the jaw (leading to blocked pores there). The good news: comedonal acne is generally addressed by keeping pores clean and open, regular gentle exfoliation (with salicylic acid, for example) and avoiding heavy pore-cloggers (I’ll list those later) can help a lot. They are precursors to inflammatory acne, if bacteria infiltrate a whitehead, it can turn into a red pimple. So tackling comedones early can prevent later breakouts.
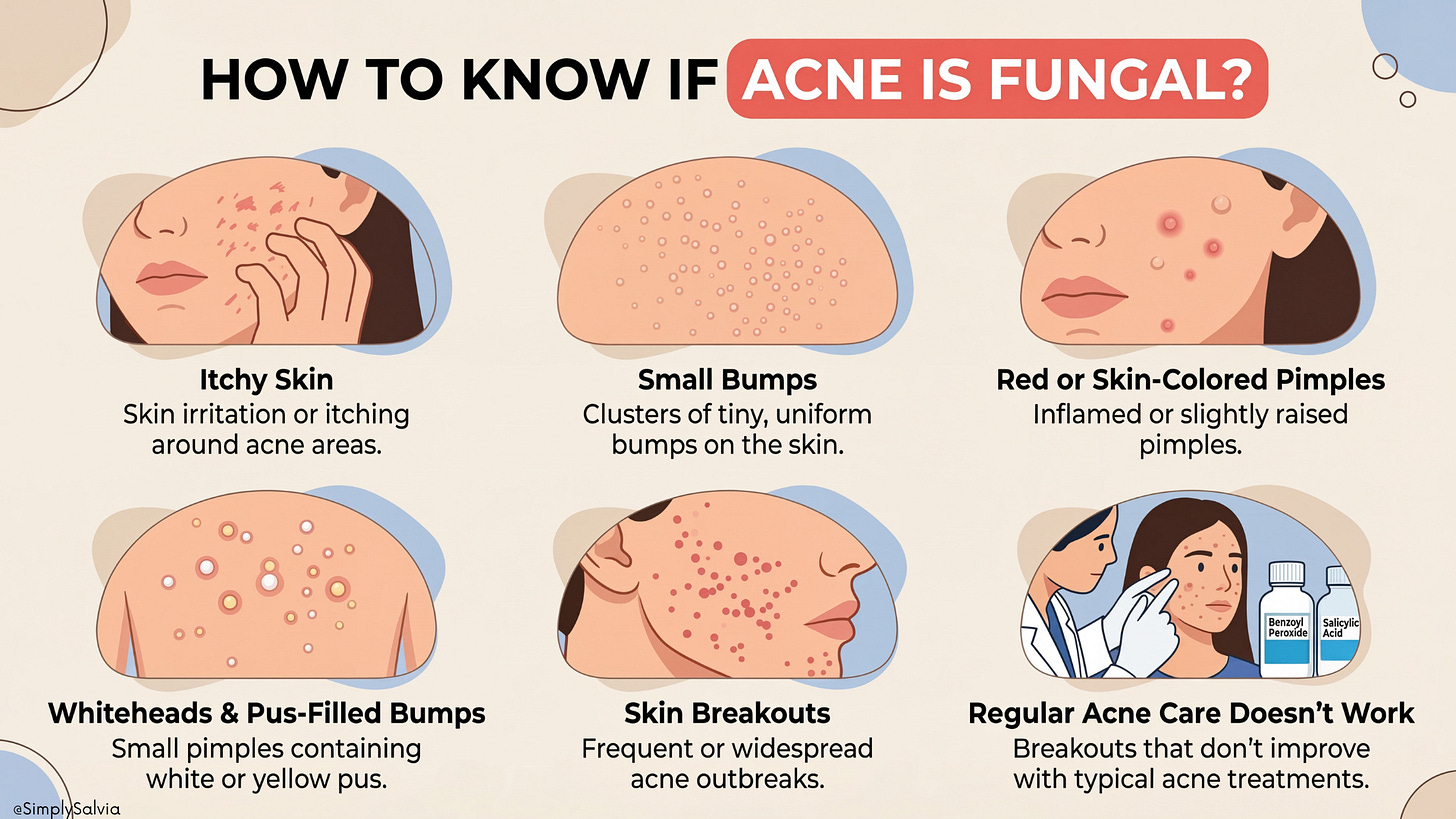
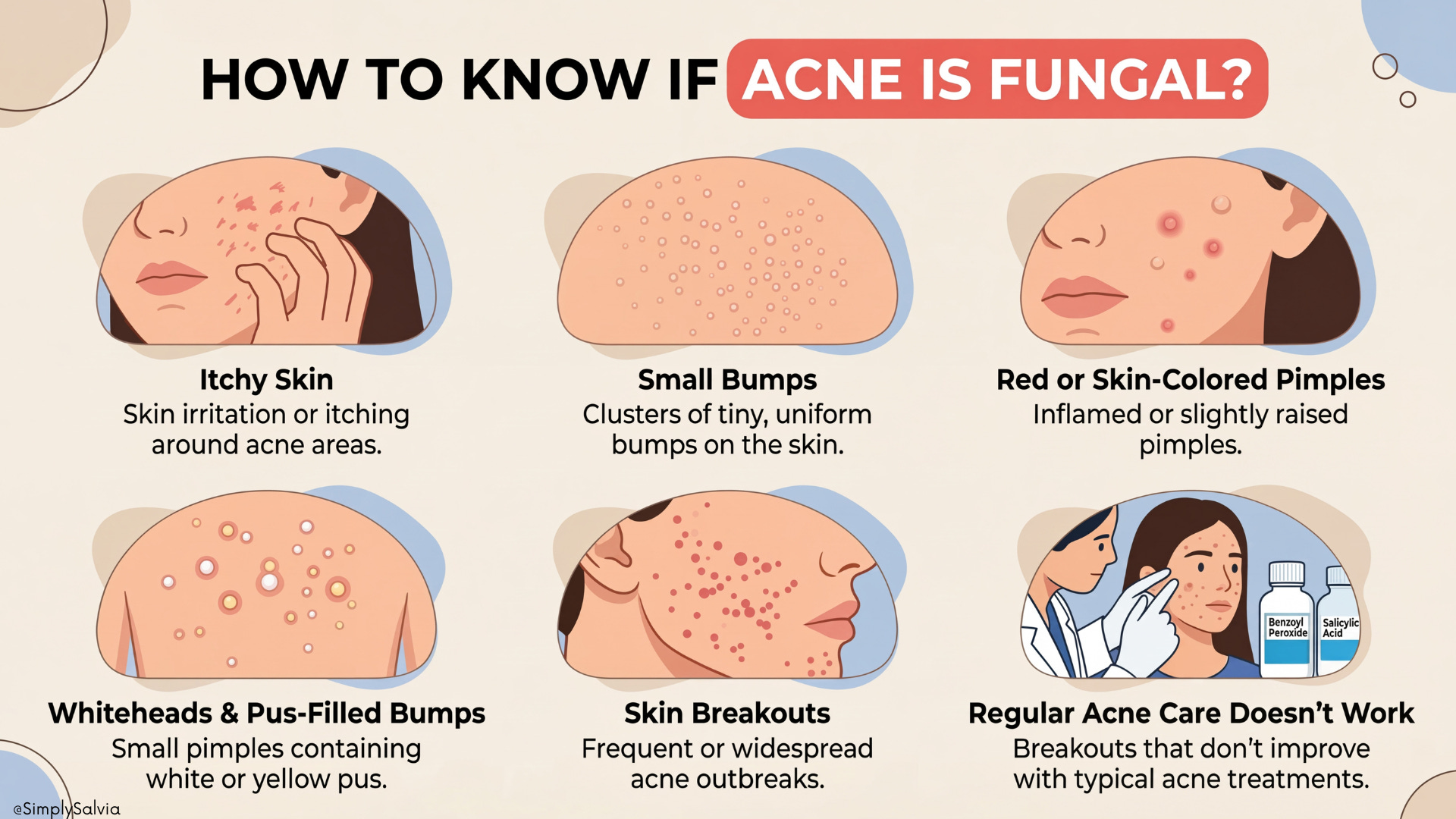
Fungal Acne (Malassezia Folliculitis): Despite the nickname, fungal “acne” isn’t true acne at all rather it’s an overgrowth of yeast (Malassezia) in the hair follicles. It produces monomorphic (all similar-looking) pinhead sized bumps, often itchy and often in clusters. A key difference: fungal folliculitis pimples tend to all be about the same size and may have a fine whitehead; they’re frequently seen on areas like the forehead, hairline, chest, and back, but can appear along the jawline especially in hot, humid conditions or if you’ve been sweating under a mask/helmet. One big differentiator is itching, fungal bumps itch, whereas typical acne usually doesn’t itch (it might hurt, but not itch). Also, fungal bumps don’t usually respond to standard acne meds, but they improve with antifungal treatments (like ketoconazole shampoo used as a face wash, or oral antifungal medication). If you notice your “acne” is uniform, itchy, and flares after, say, working out in a hot environment, you might be dealing with Malassezia. And yes, you can have fungal and bacterial acne simultaneously (making diagnosis tricky). Dermatologists can do a simple test with a scrape or a special UV light to confirm fungus. Why include it here? Because sometimes what we think is jawline acne (especially little bumps under the jaw or around the chin) is actually folliculitis from yeast, particularly if you’ve been on antibiotics which kill bacteria but allow yeast to overgrow. The treatment differs (antifungals vs. antibacterials), so it’s useful to recognize.
Acne + Oily Skin vs. Acne + Dry/Sensitive Skin: This is often categorized by lesion type, but another important distinction is overall skin type. Oily, acne-prone skin is very common; excess sebum, shiny face by midday, and frequent clogged pores. People with oily skin can usually tolerate stronger acne treatments (like foaming cleansers, higher-dose acids) because their skin has a robust lipid barrier (though you still must be careful not to overstrip it). The acne here is driven by the surplus oil and needs oil-control strategies. On the flip side, dry or sensitive skin with acne is a bit paradoxical but it happens for example, an adult who has drier skin (or someone who’s dried their skin out with acne products) yet still breaks out. This type of acne might manifest as smaller, rashy pimples or just a few persistent spots, and the skin around is often flaky or easily irritated. Treating acne on dry/sensitive skin is tricky because many acne meds are drying (retinoids, benzoyl peroxide). If this is you, the focus should be on gentle balancing: using moisturizers (yes, even though you have acne!) and milder active ingredients. Often acne in dry skin is related to inflammation and a damaged skin barrier rather than huge oil production. Some people even develop “dry acne” from using harsh products that strip the skin, the skin reacts by both being dry and breaking out (often due to secondary inflammation).
The key difference is how your skin feels: if it’s often tight, easily reddened, or flaking, you have dry/sensitive skin that needs care. If it’s consistently shiny, thick-feeling, and rarely irritated by products, you’re in the oily camp. Both types can get jawline acne, but the approach (products and routines) will differ. For instance, an oily-skin acne routine might include a salicylic acid cleanser and clay masks, whereas a dry-skin acne routine might favor a creamy cleanser and niacinamide serum plus lots of hydration. Remember: even oily skin can be dehydrated (lacking water), so hydration is important for all. And even dry skin can get clogged (especially from rich creams). So find that balance.
Recognizing these acne types in yourself can help tailor your game plan. Many people have a mix e.g., hormonal cysts on the jaw, blackheads on the nose, and a few pustules on the cheeks. That’s okay; you may just spot-treat different areas appropriately. The rest of this short dive will focus on jawline/hormonal acne, but keep these distinctions in mind as you tweak your regimen.
You now know something most women who’ve been fighting their jawline for years still don’t.
That the breakout isn’t random. That it maps to a hormonal pattern that’s specific, biological, and most importantly, addressable. That cystic and comedonal acne aren’t just different severities of the same thing; they’re different conditions that need different approaches. That for some women, the jawline is a symptom of something systemic running underneath — PCOS, insulin resistance, thyroid dysfunction and no serum is ever going to touch that.
Part 1 was the why. Part 2 is the what now.
And this is the part that most acne content either gets wrong or leaves out entirely.
Chapter 5 goes through your current skincare and makeup labels ingredient by ingredient — the specific compounds that are clinically comedogenic and may be causing breakouts without you ever connecting them to the product.
Chapter 6 covers the natural remedies and topical approaches that have actual research behind them for hormonal acne specifically and not just “gentle skincare,” but what to use, in what order, and why it works for this type.
Chapter 7 is the lifestyle and supplement chapter — spearmint, zinc, omega-3s, the herbal teas with clinical evidence, and the daily habits that directly influence sebum production and androgen activity.
Chapter 8 is the diet deep-dive: the glycaemic index research, the dairy-acne connection (more specific than you’ve been told), and the anti-inflammatory foods that show up consistently in the dermatology literature.
Chapter 9 is the one to bookmark: the signs that mean this has moved beyond DIY, what to actually ask your doctor, and why hormones tested is different from hormones mentioned in passing at a GP appointment.
Plus a complete action plan — this week, this month, ongoing, so nothing gets lost.
The calendar breakout is a pattern. Patterns can be interrupted.
Upgrade to read Part 2 →
References:
Ada Health. What are the causes of acne? (2025) – Explains how hormones trigger sebum, and how sebum and dead cells clog pores, leading to inflammationada.comada.com.
Nebraska Medicine, Dr. J. Adams. Hormones and cystic acne: what you need to know. (2020) – Notes that hormonal fluctuations (estrogen/progesterone changes) and conditions like PCOS commonly cause deep jawline acnenebraskamed.comnebraskamed.com.
Harvard Health, Liu & Nassim MD. PCOS and the skin. (2021) – Describes how PCOS-related acne is often jawline, deeper, and tied to menstrual cycles; excess testosterone and insulin resistance are underlying causeshealth.harvard.eduhealth.harvard.edu.
MDPI – Int. J. of Molecular Sci. (2024). Metabolic and Endocrine Preconditioning Associated with Acne. – Found insulin resistance and hypothyroidism were associated with more severe acne; elevated androgens and thyroid imbalances can affect sebaceous activitymdpi.commdpi.com.
Cleveland Clinic. Fungal vs. bacterial acne. (2022) – Highlights that fungal acne bumps are itchy and uniform, whereas regular acne varies and usually isn’t itchymy.clevelandclinic.org.
LATHER Skincare. How to Care for Oily or Acne-Prone Skin. (2025) – Emphasizes even dry or combination skin can get acne, and notes acne happens when oil/dead skin clogs pores; oily skin often but not always coincides with acnelather.com.
CodeSkin Blog. Understanding Comedogenicity. (2025) – Lists common pore-clogging ingredients (coconut oil, lanolin, isopropyl myristate, etc.) and advises checking labelscodeskin.incodeskin.in.
Pharmacy Times, A. Fero PharmD. Topical niacinamide for acne. (2024) – Notes 4% niacinamide gel was as effective as 1% clindamycin in reducing acne lesions, and niacinamide lowers sebum and inflammationpharmacytimes.com.
Saric et al., Green Tea Polyphenols and Sebum Production. Antioxidants (2017) – Review finding that topical green tea (EGCG) can reduce sebum and improve mild acne, due to anti-androgen and anti-inflammatory effectsmdpi.commdpi.com.
Verywell Health, L. Dorwart. Spearmint Tea for Acne. (2025) – Summarizes studies showing spearmint tea can decrease testosterone and possibly improve hormonal acne in PCOSverywellhealth.com.
Dermatologist NYC Blog. Adult Acne Triggers. (2023) – Recommends low-glycemic diet (high GI foods and dairy can worsen acne) and notes a 44% higher acne risk with milk consumption; also stress worsens acne for majority of peopledermatologist-nyc.comdermatologist-nyc.com.
Cureus Journal (Meta-analysis RCTs, 2023). Probiotics on Acne. – Concludes probiotics use was associated with reduced acne severity, particularly fewer comedones, likely by modulating inflammation and the gut-skin axiscureus.comonlinelibrary.wiley.com.
News-Medical (L. Thomas, MD). Omega-3 fatty acids reduce acne. (2024) – Reports ~80% of patients saw improved acne severity on omega-3 supplementation, plus better quality of lifenews-medical.net.
Int J Dermatology (2020). Zinc Therapy for Acne – Meta-analysis. – Confirms that acne patients have significantly lower serum zinc and that zinc supplementation can effectively reduce inflammatory acne lesionsfrontiersin.orgfrontiersin.org.
Nebraska Medicine. When to see a dermatologist for cystic acne. (2020) – Advises that if cystic acne risks scarring or isn’t responding to routine care, see a board-certified dermatologist for individualized treatment (e.g., retinoids, hormonal therapy)nebraskamed.com.