

Short Dive: Why Your Hair Is Falling Out, And What Actually Helps
The honest, research-backed guide to hair loss in women that nobody seems to have written yet.

The first time I noticed it I was brushing my hair and the brush came away with more than it should. I told myself it was fine. Normal shedding. Everyone loses hair.
Then it was the shower drain. Then the pillow. Then the ponytail that felt noticeably thinner in my hand than it used to. By the time it was obvious enough to worry about, it had been happening for months.
This is how hair loss usually goes for women. Quietly at first, then all at once. And the information available when you finally start looking? Either terrifying, or trying to sell you something.
This short dive is the guide I wanted then. What’s actually happening. Why it happens to women specifically. What the research says works and what it says about the expensive supplements and serums that dominate this space. And, the practical framework: the blood tests to ask for, the treatments with real evidence, and the honest timeline.
Let’s start with the biology.
Chapter 1: How Hair Actually Grows And Why That Determines Everything
The Hair Cycle
Every single hair on your head is going through its own independent cycle -completely separate from the hairs around it. And understanding this cycle is the key to understanding why hair loss happens the way it does: why it’s delayed, why it’s diffuse, and why recovery takes so much longer than you’d expect.
The cycle has three phases:
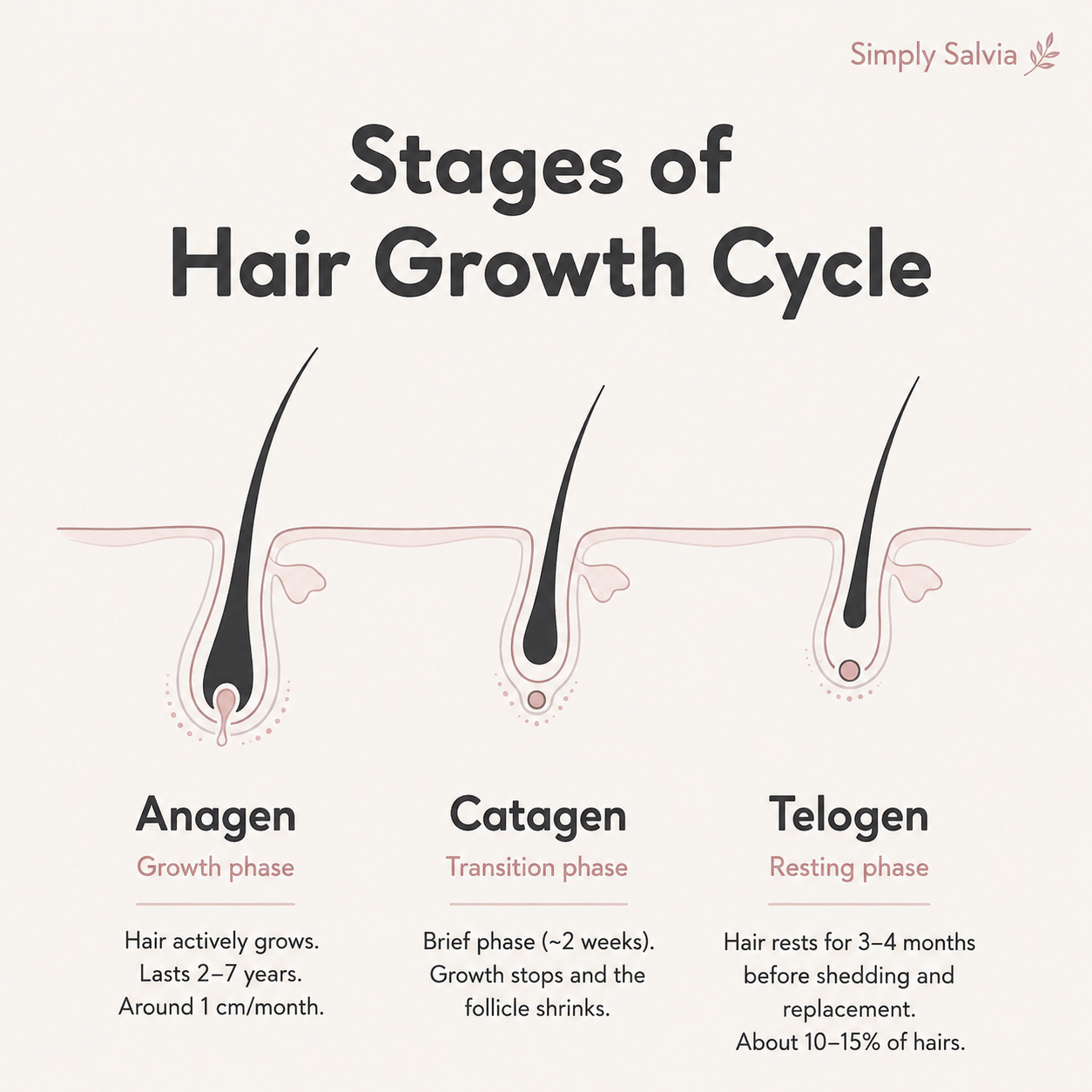
Anagen: the growth phase
This is when the hair is actively growing. Each strand spends between two and seven years in anagen, growing approximately 1cm per month. The length your hair can reach is largely determined by how long your follicles stay in anagen, which is partly genetic.
Catagen: the transition phase
A brief two-week window where the hair stops growing and the follicle starts to shrink and detach from its blood supply. Only about 1% of hairs are in this phase at any given time.
Telogen: the resting phase
The hair is no longer growing but is still attached to the follicle. It stays here for approximately three to four months before being shed and replaced by a new anagen hair growing underneath. About 10–15% of your hairs are in telogen at any one time.
Normally losing between 50 and 100 hairs per day is considered completely normal. These are the telogen hairs that have completed their cycle. The reason you don’t go bald is that only a small percentage of follicles are in this phase at any time, and the majority are actively growing.
Why Hair Loss Is Always Delayed
Here’s the thing that catches almost everyone off guard: whatever caused your hair loss happened two to three months before you noticed it.
When something goes wrong whether it’s a physical stressor, a hormonal shift, an illness, a period of severe restriction, a crash diet. The body’s response is to push a large number of hair follicles out of anagen and into telogen simultaneously. But those hairs don’t fall out immediately. They sit in the telogen resting phase for two to three months before they’re shed.
This means that by the time the hair is coming out in handfuls in the shower, the trigger already happened months ago. Which is why people so often struggle to identify what caused it. The event felt unrelated because it happened before the shedding started.
A 2025 review of 2,851 female telogen effluvium patients confirmed this two-to-three month delay as the consistent pattern across thousands of cases. The trigger and the shedding are temporally disconnected in a way that makes the cause genuinely difficult to identify without understanding the biology.
Normal Shedding vs. Actual Hair Loss - The Difference
The distinction matters because panic about normal shedding is common and it’s useful to know what you’re actually dealing with.
Normal shedding: Diffuse, even hair loss across the whole scalp. 50–100 hairs per day. The hair that comes out has a white bulb at the root (a telogen hair, it completed its cycle). No change in the density of your part or hairline. No patches.
Telogen effluvium (shedding disorder): More than 100–150 hairs per day, usually after a trigger. Often visible at the part line (which appears wider) or in the ponytail (which appears thinner). The hairs lost have white bulbs, they’re telogen hairs that were pushed out of their cycle early. Temporarily elevated, usually reversible.
Female pattern hair loss (androgenetic alopecia): Gradual thinning over months or years, primarily at the crown and widening of the part. The hairs lost are progressively finer and shorter, miniaturised by androgen activity at the follicle. Less diffuse than TE, more patterned. Responds to different treatments.
Alopecia areata: Patchy, often sudden hair loss in distinct circular areas. Autoimmune in origin, the immune system attacks hair follicles. Requires medical assessment.

Most young women experiencing sudden, diffuse hair shedding have telogen effluvium, which is reversible once the trigger is identified and addressed. The first job is identifying what caused it.
Chapter 2: The Most Common Causes in Women Under 35
Iron Deficiency - The Most Common and Most Missed
This is the one I most want you to know about because it’s the most common nutritional cause of hair loss in young women, the most consistently documented in research, and the most routinely missed by standard blood tests.
Iron plays a critical role inside the hair follicle. It’s required for DNA synthesis - the process that lets follicle cells divide and produce new hair. When iron stores are low, the follicle prioritises essential functions and hair production gets deprioritised. Follicles shift into telogen early, shedding increases, and new hair grows in finer and more slowly.
The important distinction: the blood test that GPs most commonly run is haemoglobin, which tests for anaemia. But you can be iron-deficient without being anaemic. Your haemoglobin can be completely normal while your iron stores are nearly empty. Only 32% of women with chronic telogen effluvium in one study were anaemic but 86% had low ferritin. Ferritin is the protein that stores iron, and it depletes long before haemoglobin falls.
A meta-analysis of 36 studies involving over 10,000 women found that those with hair loss had significantly lower ferritin levels than those without, on average 18 ng/mL lower. The critical threshold most dermatologists now use for hair loss specifically is ferritin below 40 µg/L but the standard lab reference range for “normal” ferritin often starts at 12 or 15 µg/L. This means you can receive a “normal” result while sitting at a level that’s driving hair loss.
Women aged 15–35 are disproportionately affected because of menstrual blood loss. Menstruation depletes iron monthly, and if dietary intake isn’t replacing what’s lost, which is genuinely difficult without red meat on a typical Western diet, ferritin gradually depletes over months or years. Iron deficiency affects approximately 72% of women experiencing hair loss, making it the single most common underlying factor.
What to do: Ask for ferritin specifically and not just a full blood count or haemoglobin. Ask what your result is rather than just whether it’s “normal.” If it’s below 40 µg/L, discuss iron supplementation with your GP.
Dietary iron: red meat is the most bioavailable source; lentils, chickpeas, spinach, pumpkin seeds, and sardines for plant-based sources. Always pair plant-based iron with vitamin C. Avoid tea and coffee within an hour of iron-rich meals.
Stress - The Mechanism Is More Specific Than You’ve Been Told
Stress-related hair loss is real, documented, and follows a predictable biological pattern. But “stress causes hair loss” is too vague to be useful. Here’s the specific mechanism.
Cortisol (the main stress hormone) affects hair follicles directly. A 2025 paper in JAAD Reviews detailed how cortisol, the HPA axis, inflammatory cytokines, and neuropeptides mediate telogen effluvium and found a particularly cruel feedback loop: stress triggers TE, but the psychological distress of watching your hair fall out maintains and amplifies the stress response that caused the shedding. The hair loss and the stress feed each other.
When the body is under significant stress, approximately 70% of anagen hairs can be pushed into telogen simultaneously far more than the usual 10–15%. This produces the alarming shower-drain level of shedding that most people don’t connect to the period of burnout or acute stress that happened two months earlier.
Both acute stress (a major life event, illness, surgery) and chronic stress (sustained work overload, long-term sleep disruption, ongoing emotional strain) can trigger TE but they do so through overlapping mechanisms. A 2025 Cureus review identified a newly understood pathway: chronic psychological stress impairs mitochondrial function in follicular cells, accelerating the shift out of the growth phase through oxidative stress. This is a structural cellular effect, not just a “stress response.”
The good news: Stress-triggered TE is almost always reversible. Once the trigger is removed and the body recovers, follicles return to anagen. Shedding typically slows within three to six months after the stressor resolves, and regrowth begins. Full cosmetic recovery takes 12 to 18 months, because hair grows slowly regardless of how well the follicles are functioning. The timeline is longer than most people expect, which creates the impression that recovery isn’t happening when it actually is.
Hormonal Shifts; Postpartum, Post-Pill, and the Cycle

Postpartum hair loss is the textbook example of hormonally triggered TE. During pregnancy, estrogen rises significantly and keeps a much higher percentage of hairs in the anagen (growth) phase, which is why many women’s hair is thicker and more lustrous when pregnant. After birth, estrogen drops sharply. The hairs that were held in anagen by elevated estrogen all transition to telogen simultaneously. Two to four months later, the shedding arrives and for new mothers in an already exhausted, depleted state, it can be severe.
Postpartum TE is almost universally self-resolving. The follicles are healthy. The trigger; the hormonal shift was a one-time event. Given adequate nutrition (particularly iron and protein, which are often depleted in the postpartum period), recovery is the expected outcome.
Post-pill shedding follows the same mechanism. The combined oral contraceptive pill maintains artificially elevated synthetic hormones. When it’s stopped, those hormones drop and the hair that was held in anagen by the pill’s hormonal environment transitions to telogen. The shedding typically begins six to twelve weeks after stopping the pill and can last three to six months. Again, self-resolving once the body establishes its natural hormonal rhythm.
The menstrual cycle and hair shedding is a less discussed but real phenomenon. Research published in the British Journal of Dermatology examining 17,009 women found significant skin and hair condition changes associated with menstrual cycle irregularity. The luteal phase (the two weeks before the period) is when estrogen is falling and progesterone is dominant. Some women notice increased shedding in this window. This is hormonal fluctuation affecting the follicle environment at a cycle level rather than a structural hair loss condition. Notably worse in the context of iron deficiency, which amplifies the follicular sensitivity.
PCOS creates chronic androgen excess (elevated testosterone and DHT) which miniaturises hair follicles on the scalp (androgenetic alopecia pattern) while simultaneously causing excess hair growth elsewhere. If hair loss follows a pattern of central and crown thinning with widening of the part, and you have other PCOS symptoms (irregular cycles, acne, excess body hair), this is the conversation to have with a GP.
Other Causes Worth Knowing
Thyroid dysfunction: Both hypothyroidism (underactive) and hyperthyroidism (overactive) are associated with diffuse hair loss. The thyroid regulates cellular metabolism, including the metabolic activity of hair follicles. Thyroid issues are more common in women than men and are frequently underdiagnosed. An October 2025 study of 100 women with hair loss found significantly different thyroid hormone profiles in the hair loss group compared to controls. TSH (thyroid-stimulating hormone) is the standard test; ask for this alongside ferritin if diffuse hair loss has no obvious trigger.
Rapid weight loss or severe calorie restriction: The body deprioritises hair production under significant energy deficit. This is one of the mechanisms behind TE in eating disorders and crash dieting. The follicles are not damaged, they’ve simply been put into conservation mode. Recovery requires restoring adequate nutrition and calorie intake.
Vitamin D deficiency: Increasingly documented as a contributing factor. Vitamin D receptors are present in hair follicles, and deficiency is associated with accelerated follicle miniaturisation and slower regrowth. Worth including in any hair loss blood panel.
Protein deficiency: Hair is made almost entirely of keratin - a protein. Inadequate dietary protein provides insufficient building material for hair production, particularly relevant for women on very low-calorie or low-protein diets.
Chapter 3: The Evidence Hierarchy. What the Research Says Actually Works
This chapter is the one that differs most from what’s being sold to you.
The hair loss supplement and serum industry is enormous. Biotin gummies, collagen powders, “hair growth vitamins,” scalp serums with seventeen ingredients. The marketing is compelling and the evidence behind most of it is thin. Here’s what the research actually ranks.
What Has Strong Evidence
Minoxidil: the strongest evidence for hair growth in women
Minoxidil was originally developed as a blood pressure medication. One of its side effects was hair growth and that side effect became the treatment. It works by prolonging the anagen phase of the hair cycle and increasing blood flow to follicles, giving them a better nutrient supply.
5% topical minoxidil is FDA-approved for female hair loss. A 2025 meta-analysis of randomised clinical trials found that oral minoxidil at low doses (0.25–2.5mg daily for women) produced comparable or superior hair regrowth to topical minoxidil, with good tolerability at low doses. A JAMA Dermatology consensus statement in January 2025 from an international panel established best practice guidelines for low-dose oral minoxidil, signalling its acceptance as a mainstream treatment rather than a fringe one.
The honest caveats: minoxidil works while you use it. If you stop, hair that was maintained by it will shed again within a few months. It requires commitment to ongoing use. It also takes three to six months to show meaningful results - shorter than the recovery timeline from TE, but still requiring patience. And low-dose oral minoxidil requires a GP prescription and cardiac screening for anyone with a relevant medical history.
Addressing the underlying cause first. If hair loss is driven by iron deficiency, no topical treatment will fully compensate. Restoring ferritin is the primary intervention and once levels are adequate, the follicles resume normal function. Same logic applies to thyroid dysfunction, severe dietary restriction, and hormonal disorders. The treatment must match the cause.
What Has Reasonable Evidence

Iron supplementation (when deficient)
Not as a supplement for everyone (iron toxicity is a real risk) but for women with confirmed low ferritin, supplementation is well-evidenced for supporting hair regrowth. The form matters: ferrous fumarate or ferrous sulfate are well-absorbed; ferrous gluconate is gentler on the stomach if the others cause GI issues. Taken with vitamin C, away from tea and coffee.
Zinc
Hair loss patients consistently show lower zinc levels than controls. The October 2025 study of 100 women with hair loss found significantly lower zinc in the hair loss group. Zinc plays a role in follicle cell division and the hair growth cycle. However, excessive zinc supplementation suppresses copper absorption and can cause its own problems, supplementation should be guided by blood levels rather than taken speculatively.
Vitamin D
As above - worth testing, worth supplementing if deficient. 1,000–2,000 IU daily is well-evidenced as safe for most adults at low to moderate deficiency.
What the Research Doesn’t Strongly Support

Biotin
The biotin-hair growth connection is one of the most heavily marketed claims in the supplement industry.
The evidence: biotin deficiency (genuinely rare) is associated with hair loss, and correcting it helps. But supplementing biotin above adequate levels in people who are not deficient has no demonstrated effect on hair growth or retention. Most people consuming a typical diet are not biotin-deficient. Biotin supplements are being purchased on the basis of a mechanism (deficiency = hair loss) that doesn’t apply to the people buying them. They also interfere with thyroid and cardiac blood tests.
Collagen supplements for hair growth
Collagen provides amino acids that are building blocks for hair keratin. The indirect logic makes sense. The clinical evidence for oral collagen supplementation specifically producing measurable hair growth is thin. There are better and cheaper ways to get protein.
Most proprietary “hair growth vitamin” blends
Usually contain biotin (not evidenced for non-deficient individuals), some B vitamins (useful only if deficient), and various botanicals (saw palmetto, DHT-blocking herbs) at doses too low to produce the effects claimed. Save the money for ferritin testing or an actual treatment.
Scalp serums with “growth-stimulating” ingredients (rosemary oil, caffeine serums, peptides)
Some preliminary evidence exists for rosemary oil, one small study found it comparable to 2% minoxidil at 6 months. It’s not evidence of strong efficacy; it’s evidence that it might do something. Caffeine applied to the scalp has some in-vitro evidence for blocking DHT at the follicle. None of this is at the level of minoxidil evidence. These can be incorporated into a routine, but they are not treatments.
Part 1 ends here. Part 2 is the practical half: the blood tests to request, the full treatment guide, the supplement breakdown, how to build a recovery routine, and the cycle-aware approach for the weeks when shedding is reliably worse.
Now you understand what’s actually happening. The hair cycle and why loss is always delayed. The causes most common in women under 35; iron deficiency (the one most GPs miss), stress (with a more specific mechanism than you’ve been told), hormonal shifts, and thyroid. And the evidence hierarchy for treatment, which looks very different from what the supplement industry presents.
Part 2 takes all of this and makes it actionable.
Chapter 4 is the blood test guide. Exactly what to ask for, what the numbers mean, and what the targets are for hair health specifically versus the standard “normal” ranges.
Chapter 5 is the full treatment guide. Minoxidil in detail (topical versus oral, what to expect, the timeline), what the hormonal treatments do, and the honest assessment of every other intervention in the space.
Chapter 6 is the supplement chapter. What the evidence actually says about biotin, collagen, zinc, iron, vitamin D, and the “hair growth blends,” with the specific scenarios where each one makes sense and the ones where you’re wasting money.
Chapter 7 is the cycle-aware approach. How to support your follicles in the weeks where shedding is hormonally worse, what dietary and lifestyle interventions the research backs for the luteal phase specifically.
Chapter 8 is the complete practical guide: the daily routine for hair health, what to do in months one through twelve, and when to stop trying to manage this yourself and see a dermatologist or trichologist instead.
Subscribe to read Part 2 →
Sources & Further Reading
Hughes, Syed & Saleh. Telogen Effluvium — StatPearls, NIH, 2024 update
Shapiro Medical. Hair loss from stress and telogen effluvium — mechanism review, 2025–2026 research
Olsen et al. Summation and recommendations for topical and oral minoxidil — JAAD, August 2025
Löffler et al. Omega-3 fatty acid deficit in acne patients — PMC, 2024