

Short Dive: Everything You’ve Been Told About Weight Loss Is Half the Story
The calorie deficit is real. The hunger hormones are real. The reason it’s harder for women is real. Here’s what the research actually says and the part nobody is talking about.

I want to start with something that might sound obvious but actually isn’t.
Weight loss is not complicated because people don’t know what to do. It’s complicated because the advice that exists was mostly built around men’s bodies and then handed to women without any adjustments. The calorie counts, the macros, the meal timing, the exercise prescriptions. Most of it comes from research conducted primarily on men and applied universally.
This matters because women’s bodies don’t work the same way. Not because they’re broken or more difficult. But because estrogen, progesterone, and the hormonal cycle create a completely different metabolic environment — one that affects how much you eat, how much you store, how hungry you are, and how quickly you lose. The research is only starting to catch up.
What this Short Dive is going to do is give you the honest, research-backed version of what weight loss actually involves for a woman’s body. Not the calorie-counting app version. Not the influencer version. The part that explains why you’ve done everything “right” and still felt like your body wasn’t cooperating and what to actually do about it.
Three chapters in Part 1. The rest in Part 2. Let’s go.
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
PS: We also have a subscriber-only group chat where members discuss the deep dives, share their sleep journeys, and ask me questions directly. See you there.
Disclaimer: The information and opinions expressed above are current as of the date of this post and are subject to change without notice. Materials referenced above are provided for educational and informational purposes only. None of the above constitutes medical advice, a diagnosis, a treatment recommendation, or a substitute for consultation with a qualified healthcare professional. Always seek the guidance of your doctor or another qualified health provider with any questions you may have regarding a medical condition or sleep disorder.
Short Dive below ↓
Table of Contents:
What Weight Loss Actually Is And Why Your Body Pushes Back
The GPL Framework — Why What You Eat Matters as Much as How Much
Why Your Hunger Isn’t a Willpower Problem
Chapter 1: What Weight Loss Actually Is And Why Your Body Pushes Back
The Part That’s True
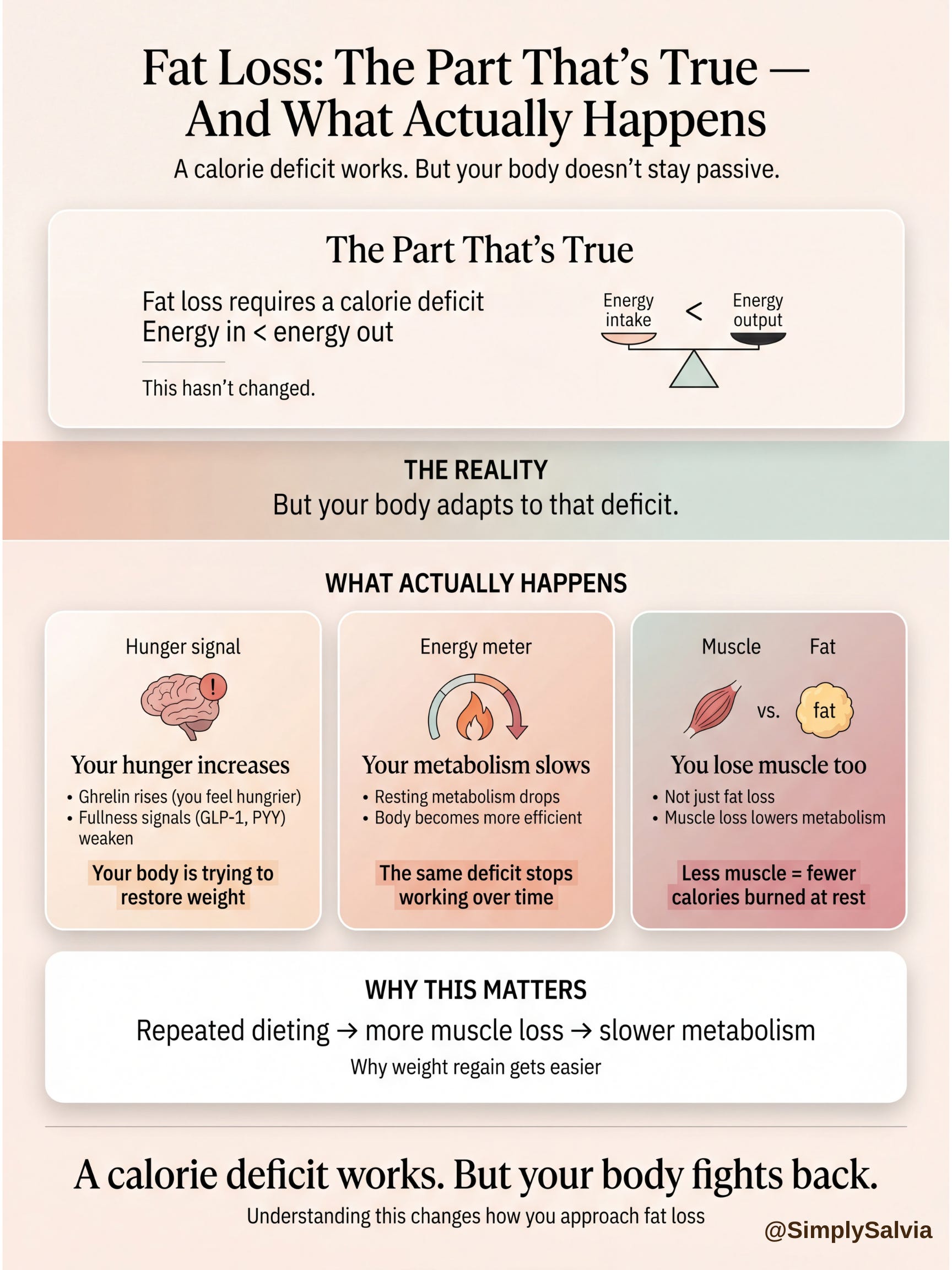
Yes, a calorie deficit is required for fat loss. This is one of the most well-established findings in nutrition science and it hasn’t changed. To lose fat, you need to consume less energy than your body is using. That’s it.
But the way that’s been communicated; “eat less, move more,” 500 calories less per day, one pound per week, clean and simple — misses so much of what actually happens in a body when you try to do that.
Here’s what the research shows actually happens when you reduce your food intake:
Your Hunger Hormones Change
Ghrelin (the hormone that tells your brain you’re hungry) rises when you’re in a calorie deficit. This isn’t a character flaw or a lack of willpower. It’s your body doing exactly what it was designed to do: fighting to bring you back to your previous weight. Research published in 2024 in the journal Current Opinion in Endocrinology confirmed that gut hormones including ghrelin, GLP-1, and PYY are the primary drivers of appetite regulation, and that in a deficit, ghrelin rises while the hormones that make you feel full (GLP-1 and PYY) become less effective.
Your Metabolism Adapts
Your body is remarkably good at adjusting to less food. When you eat less for long enough, your resting metabolic rate (the amount of energy your body burns just existing) can drop. This is sometimes called “metabolic adaptation.” It’s why the deficit that worked in week one stops working by week eight. It’s not that you’re doing it wrong. It’s that your body has literally become more efficient.
You Lose Muscle As Well As Fat
This is the part of calorie restriction that doesn’t get talked about enough. When you cut calories without doing resistance training, a significant portion of what you lose isn’t fat — it’s muscle. A January 2026 study from Tel Aviv University published in Frontiers in Endocrinology found that people who dieted without any exercise had the worst fat-to-muscle-loss ratio of any group tested. Aerobic exercise improved it. Resistance training improved it the most, to the point where the resistance training group actually lost a higher proportion of fat compared to lean muscle than any other group.
Why does losing muscle matter for weight loss? Because muscle burns more calories at rest than fat does. Every kilogram of muscle you lose makes your metabolism slightly slower. Which means the more times you’ve crash dieted and regained the weight, the harder your body works to hold onto fat and lose muscle next time — a documented phenomenon sometimes called “yo-yo dieting” that has real metabolic consequences.
Why Women’s Bodies Are Different
This is the conversation that most weight loss content skips entirely.
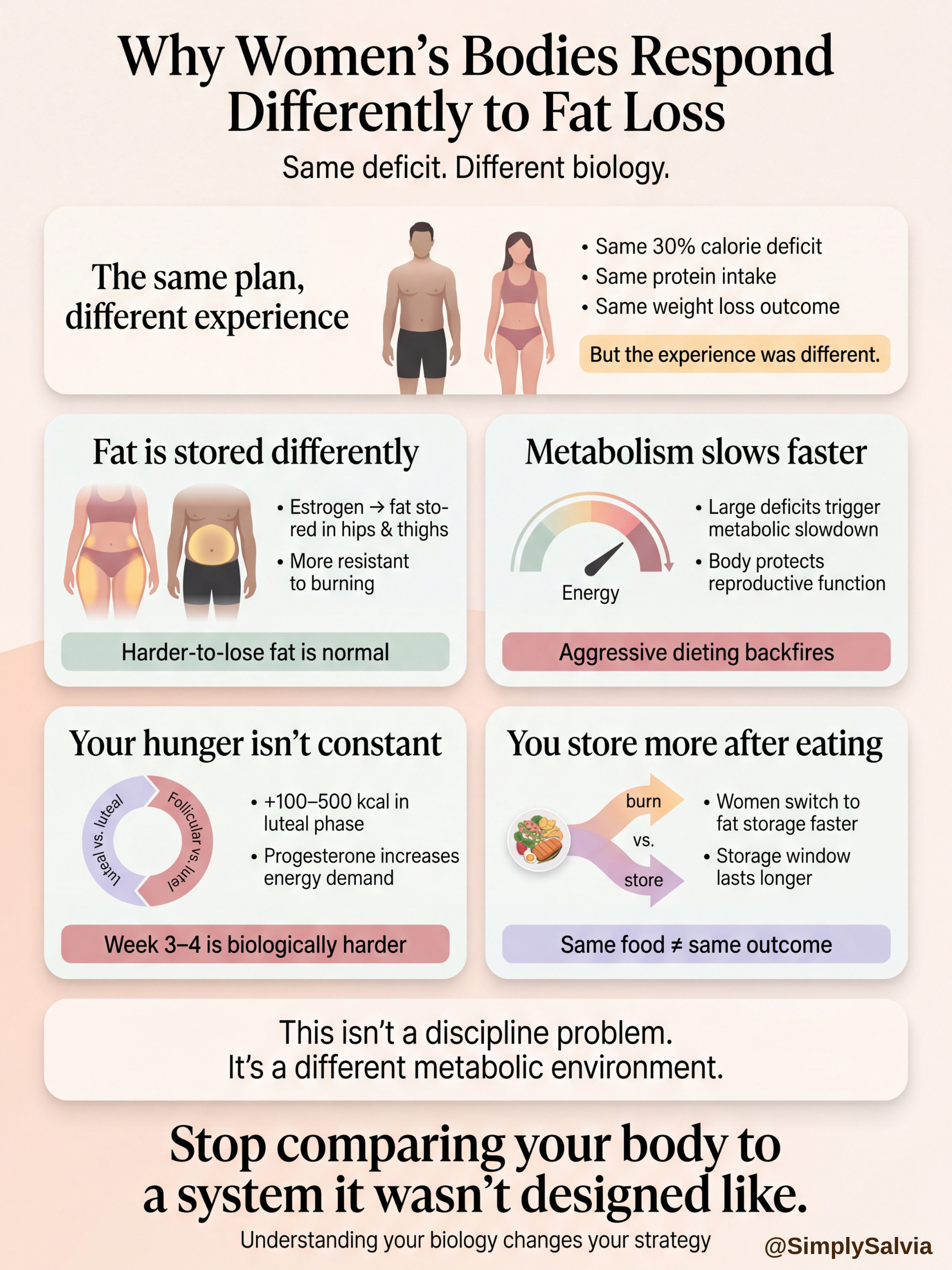
A 2025 study published in the Journal of the International Society of Sports Nutrition put 323 people (83% women) on an identical 30% calorie deficit with the same protein prescription and tracked how long it took to lose 5% of their body weight. Men and women lost weight at the same overall rate but the experience getting there was measurably different, and the research notes clearly that women’s hormonal profiles create a distinct metabolic environment.
Here’s what we know about why women’s bodies respond differently to calorie restriction:
Estrogen Promotes Fat Storage In Specific Places
Estrogen encourages fat to be stored around the hips and thighs (subcutaneous fat that sits under the skin). This fat is less metabolically active than visceral fat (the belly fat men tend to accumulate) and more resistant to being burned. This is not a design flaw. It’s an evolutionary adaptation related to reproductive function. But it does mean that hip and thigh fat is genuinely harder to shift than abdominal fat and that the comparison to a male friend or partner who’s “doing the same thing” and losing faster is not a fair comparison.
Women’s Metabolic Rate Drops Faster In A Large Deficit
Research found that when calorie intake is restricted too aggressively, women’s bodies slow their metabolism to preserve reproductive function — a protective mechanism that’s absent or much weaker in men. This is why aggressive 1200-calorie diets are counterproductive for most women: they produce the fastest initial loss and the most severe metabolic adaptation, making long-term maintenance nearly impossible.
Hunger And Appetite Change Across The Menstrual Cycle
Studies have consistently found that caloric intake increases by 100–500 calories per day in the luteal phase (the two weeks before your period). This is driven by progesterone raising metabolic rate and the body genuinely needing more fuel. Eating more in this phase is not a failure. It’s biology. But it does mean that week three and four of the month are reliably harder and any weight loss approach that doesn’t account for this will feel randomly inconsistent, because the calorie needs are genuinely different week to week.
Women Store More Fat After Eating
Research published in PMC found that after eating, women switch to fat-storage mode faster than men, and that the post-meal fat storage window lasts longer. Men burn more ingested fat after eating. Women store it more efficiently during non-exercising periods, even when eating the same foods in the same amounts. This is the biology behind the experience of feeling like you can’t eat the same things as the men around you without different results.
What This Means Before You Do Anything Else
The practical implications of all of this come down to three things:
Don’t Go Too Aggressive
A deficit of 300–500 calories per day is the range supported by research for sustainable fat loss with minimal metabolic adaptation. More than this produces faster initial results and faster metabolic slowdown; the trade-off isn’t worth it. The research points to 0.5–1kg per week as the rate at which you lose primarily fat rather than muscle.
Resistance Training Is Not Optional
This is the single most consistently supported finding in weight loss research for women. The Tel Aviv study found that resistance training produced the highest fat-to-muscle loss ratio of any group, meaning more of the weight you lose is actually fat. It also preserves the muscle that keeps your metabolism functioning. 2–3 sessions per week of resistance training is enough to produce this effect alongside a calorie deficit.
Expect Variation Across Your Cycle
If you track your intake or weight, understanding that the luteal phase reliably drives higher hunger and slightly higher water retention will prevent the last two weeks of every month from feeling like the process is breaking down. It isn’t. It’s your hormones.
Chapter 2: The GPL Framework — Why What You Eat Matters as Much as How Much
The GPL framework: Glucose, Protein, Lipids, is a way of thinking about macronutrients not as numbers to hit but as levers that directly affect hunger, hormones, and how your body decides what to store versus burn. It’s not a named clinical protocol with its own RCTs. But the individual components are among the best-supported areas of nutrition science for weight management.
This chapter is about the three levers and why each one matters.
G — Glucose: Why Blood Sugar Stability Isn’t Just a Wellness Buzzword
Blood sugar stability is one of those topics that wellness content has turned into a vague aesthetic — Glucose Goddess, green vegetables before carbs, dramatic CGM graphs. Some of it is overstated. But the underlying biology is genuinely relevant to weight loss, and here’s why.
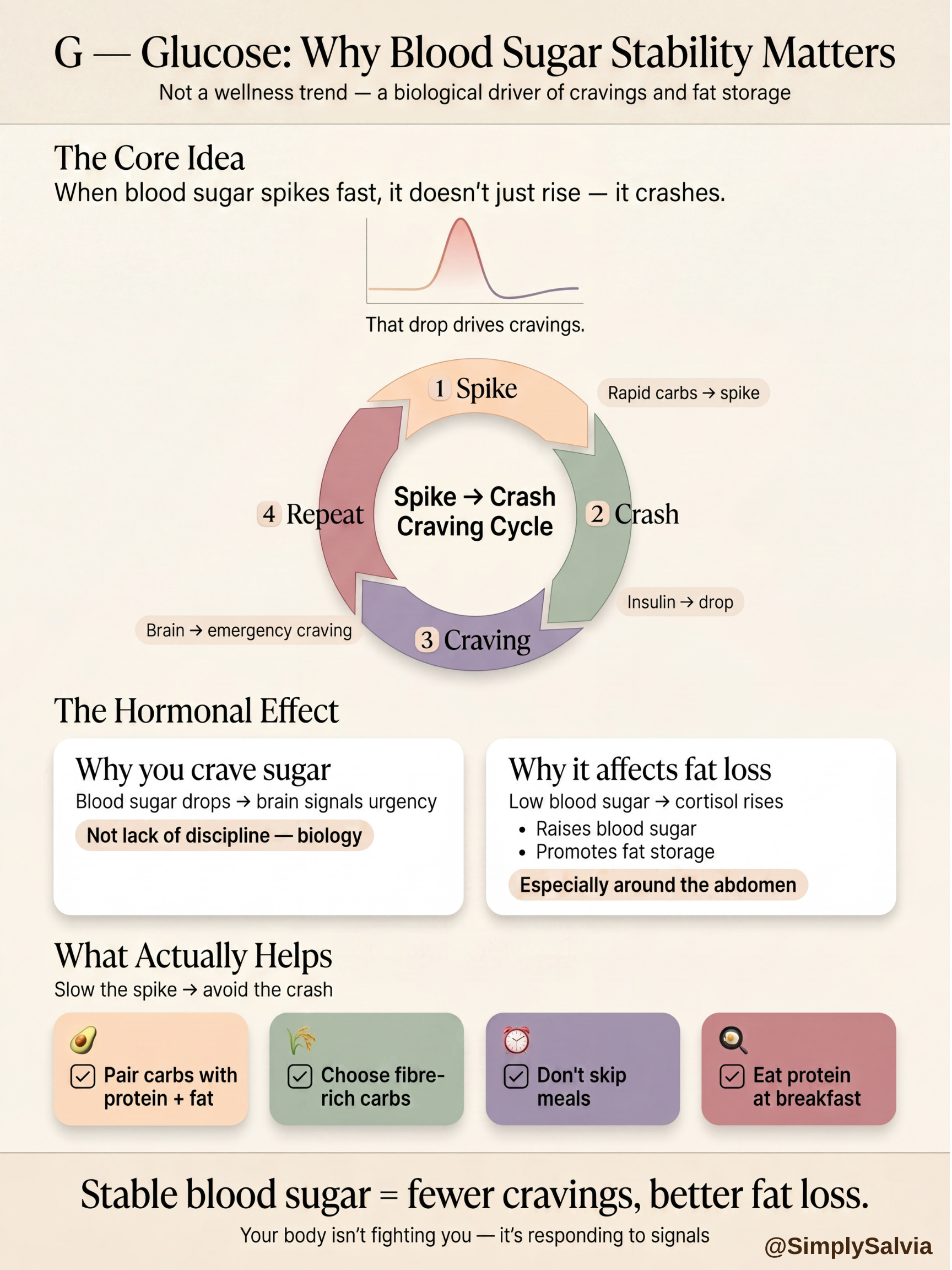
When you eat carbohydrates especially refined ones with no fibre, protein, or fat to slow them down, your blood sugar rises quickly. Your body releases insulin to bring it back down. If the spike is large, the correction can be aggressive, bringing blood sugar below where it started. That drop is what your brain experiences as a craving: specifically, a craving for fast sugar that will bring it back up again quickly. This is not psychological. It’s a direct biochemical response to a blood sugar crash.
The cycle this creates; spike, crash, craving, spike again is one of the most common reasons calorie deficits are hard to maintain. It’s not that you have no discipline. It’s that your blood sugar has been signalling an emergency and demanding a rapid fix.
Research on cortisol and blood sugar confirms another layer of this: when blood sugar drops too low, your body releases cortisol to bring it back up. Cortisol raises blood sugar through the liver. It also, when chronically elevated, promotes fat storage particularly around the abdomen. Skipping meals, eating too few carbohydrates, or crash dieting can actually elevate cortisol enough to make fat loss harder, not easier. The body experiences severe restriction as a threat and responds hormonally accordingly.
What Blood Sugar Stability Actually Requires:
Pairing carbohydrates with protein and fat to slow the digestion and reduce the glucose spike
Prioritising fibre-rich, lower-GI carbohydrates (oats, sweet potato, legumes, wholegrain bread) over refined ones
Not skipping meals as blood sugar drops are what drive the worst cravings and the cortisol response
Eating protein at breakfast specifically, research shows that high-protein breakfasts reduce glucose spikes post-meal and improve satiety significantly compared to high-carbohydrate breakfasts
The practical result of better blood sugar stability: fewer cravings, more consistent energy, less of the cortisol-driven fat storage that defeats the calorie deficit from the hormonal side.
P — Protein: The Most Important Macro for Fat Loss
Protein is the one area where the research is the most consistent and the most clear. If you change one thing about the way you eat for fat loss, it should be your protein intake.
Here’s why:
Protein Keeps You Fuller For Longer Than Any Other Macronutrient
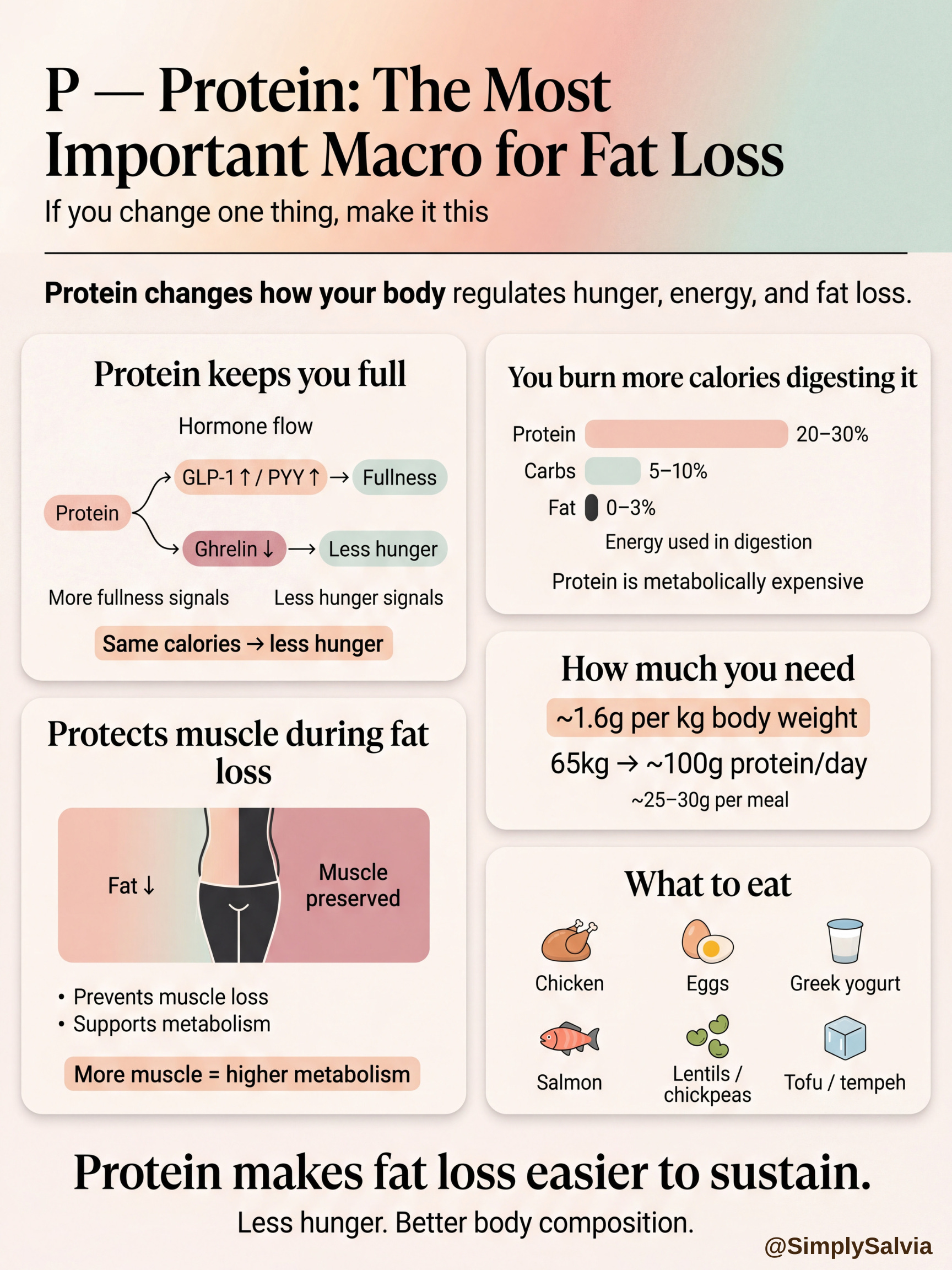
The mechanism: eating protein triggers the release of GLP-1 and PYY (satiety hormones that travel to your brain and signal that you’re full) while simultaneously reducing ghrelin, the hunger hormone. A 2025 study in Obesity Pillars examining high-protein versus high-fat snacks in women found that protein-based snacks produced stronger satiety hormone responses and greater appetite suppression than fat-based snacks. A review of the research on proteins and satiety hormones confirmed that protein is the most effective macronutrient for reducing food intake compared to both carbohydrates and fats.
GLP-1 is particularly relevant here because it’s the hormone that drugs like Ozempic mimic, the mechanism behind why those medications work so well for reducing appetite. Protein produces this same hormone naturally, though at lower intensity. Understanding this explains why a high-protein meal genuinely keeps hunger quieter than a high-carb or high-fat meal of the same calories.
Protein Has A Higher Thermic Effect
This means your body burns more energy digesting protein than it burns digesting carbohydrates or fat. Roughly 20–30% of protein’s calories are used in digestion itself, compared to 5–10% for carbs and 0–3% for fat. This isn’t a huge effect, but it does mean that a high-protein diet is slightly more energetically expensive to maintain than an equivalent-calorie lower-protein diet.
Protein Preserves Muscle
I’ve established that losing muscle alongside fat is one of the most common problems with calorie restriction. The most effective dietary strategy to prevent this is adequate protein intake. The research consensus for people in a calorie deficit doing resistance training is approximately 1.6g of protein per kilogram of body weight per day. For a 65kg woman, that’s approximately 104g of protein daily, significantly more than most women are consuming on a typical diet.
Practical Protein Sources
Chicken breast, eggs, Greek yoghurt, cottage cheese, salmon, tinned sardines, tofu, tempeh, lentils, chickpeas, edamame. The goal of 25–30g of protein per meal is achievable with these foods without supplementation, though a protein shake is a convenient way to close the gap.
L — Lipids (Fats): The Macro People Are Still Afraid Of
The fat-is-bad narrative from the 1980s and 90s is one of the most damaging pieces of dietary advice in modern history. It isn’t true, and the research has known it for decades. But it has been slow to filter into general consciousness.
Here’s what fats actually do and why they matter for weight loss:

Fat Slows Digestion And Extends Satiety
Including fat in a meal slows how quickly everything else in that meal is digested, which means the glucose spike is smaller, the satiety lasts longer, and you stay satisfied for more hours after eating. Research on how different macronutrients trigger satiety hormones confirmed that fat triggers the release of CCK (cholecystokinin), a hormone that signals fullness to the brain. Removing fat from meals in the name of reducing calories often makes meals less filling, which drives more eating later.
Fat Is Required For Hormone Production
Estrogen, progesterone, and cortisol are all synthesised from cholesterol. A diet too low in fat disrupts hormone balance. For women particularly, severely low-fat diets have been associated with irregular cycles, low estrogen, and hormonal disruption — the exact opposite of the conditions that support fat loss.
Not All Fats Are Equal
Unsaturated fats (olive oil, avocado, nuts, fatty fish) are anti-inflammatory and support metabolic health. Saturated fat in moderate amounts is not the health disaster it was presented as, but excessive intake of processed saturated fat from ultra-processed foods carries legitimate health risks. Trans fats remain clearly harmful. The framing of “fat is bad” ignored all of this nuance.
Practical Fat Intake For Weight Loss
The goal isn’t to eat as much fat as possible or to avoid it entirely. It’s to include enough fat in meals to slow digestion, support hormone production, and keep you full, while prioritising unsaturated sources. Around 25–35% of calories from fat is the well-supported range for most women.
Chapter 3: Why Your Hunger Isn’t a Willpower Problem
This chapter is short and it’s the one I most want you to actually hear.
The dominant narrative about weight loss — in media, in diet culture, in casual conversation, frames failure as a discipline problem. You ate the thing you weren’t supposed to eat. You didn’t stick to the plan. You need more willpower.
This framing ignores the physiology almost entirely.
Here’s what’s actually happening when you’re in a calorie deficit and struggling with hunger:
Ghrelin Rises And Stays Elevated
When you eat less than your body is used to, ghrelin (the hormone that tells your brain to eat) increases. This is not temporary. Research has found that ghrelin remains elevated even after significant weight loss, meaning the hunger you feel after losing 10kg is genuinely more intense than the hunger you felt before you started, driven by hormones rather than habit.
Satiety Hormones Become Less Effective
As you lose weight, the satiety signals; GLP-1, PYY, leptin, don’t work as efficiently at suppressing appetite. Your brain becomes more sensitive to food cues while the hormones that would dampen that sensitivity are less effective. This is a documented biological mechanism, not a weakness.
Your Brain Prioritises Food Seeking
Chronic mild calorie restriction activates the same reward-seeking pathways in the brain as other forms of deprivation. Research on sustained calorie restriction found that people in a deficit reported heightened focus on food, increased food-related thoughts, and reduced ability to maintain dietary restraint over time. Again: documented physiology, not lack of character.
What This Means Practically:
The goal of weight loss isn’t to fight these systems indefinitely. It’s to structure your eating in a way that works with them.
High protein at every meal because protein is the most powerful natural stimulus for the satiety hormones that resist hunger
Blood sugar stability because blood sugar crashes are hunger crises engineered by chemistry
Not too large a deficit because the larger the deficit, the more forcefully the hunger hormones respond
Resistance training because it preserves the muscle that keeps your metabolism from adapting as aggressively
Consistency without perfection because the data shows that adherence over time matters far more than the precision of any single day
Hunger during a calorie deficit is real. It is hormonal. It is not your fault. And understanding what’s driving it is the difference between fighting it blindly and building an approach that actually accounts for it.
Part 1 ends here.
Now you know the actual biology behind why weight loss is harder than “eat less, move more” and why it’s specifically harder for women. You understand what a calorie deficit actually does to your hunger hormones, why muscle loss is the hidden problem with most diets, what blood sugar stability actually means and why it matters, what protein does that no other macro does, and why your hunger is not a personal failing.
Part 2 is where all of this becomes a practical system.
Chapter 4 goes deeper into the GPL framework in practice. What a day of eating actually looks like when you’re building meals around glucose stability, protein, and fats, with specific targets and food combinations that the research supports.
Chapter 5 is the exercise chapter. The research-backed breakdown of what kind of training produces the best body composition results during a calorie deficit, how much is enough, and the cycle-syncing dimension that determines which weeks to push and which to protect.
Chapter 6 covers the things that wreck a calorie deficit from the outside; sleep, stress, alcohol, and the hormonal mechanisms behind each one. These are the invisible factors that can undo everything else, and most diet advice ignores them entirely.
Chapter 7 is the sustainability chapter. The research on what actually determines whether weight loss is maintained long term, and the specific behaviours that separate people who keep the weight off from people who regain it.
Chapter 8 is the practical guide: the weekly template, the meal framework, the tracking approach that doesn’t become obsessive, and the phase-by-phase adjustments for different weeks of your cycle.
Stay Tuned, part 2 drops next week
The information in this post is for educational and informational purposes only. None of the above constitutes medical advice, a diagnosis, a treatment recommendation, or a substitute for consultation with a qualified healthcare professional. Always seek the guidance of your doctor or another qualified health provider with any questions you may have regarding your health, weight, or nutrition.
Sources & Further Reading
Rodriguez Da Silva et al. Comparing weight loss rates between males and females — Journal of the International Society of Sports Nutrition, August 2025
Lahav, Yavetz & Gepner. Resistance training as a key strategy for high-quality weight loss in men and women — Frontiers in Endocrinology, January 2026
Systematic review and meta-analysis: resistance exercise during dietary weight loss — BMJ, 2025
Chen et al. Time-restricted eating in overweight and obese women — Frontiers in Nutrition, September 2025
Hong & Choi. Gut hormones and appetite regulation — Current Opinion in Endocrinology & Diabetes and Obesity, 2024
Al-Bayyari et al. Effects of high protein versus high fat snacks on satiety, gut hormones and insulin secretion in women — Obesity Pillars, September 2025
Proteins and Peptides with Effect on Satiety — PMC, October 2024
Sex Differences in Energy Metabolism — PMC