

Short Dive: Why Your Neck and Shoulders Are Always Tense. And What to Actually Do About It (Part 1)
It's not just bad posture. Your nervous system is involved — here's how to release it.

At some point, it stopped feeling like a symptom.
The tightness across the top of your shoulders that’s just there when you wake up. The neck that crunches when you turn it too fast. The dull ache that starts behind one shoulder blade and travels up into your skull by 4pm. The headache that isn’t quite a headache — more like a vice, starting at the base of your neck and pressing forward. You don’t mention it anymore because there’s nothing to mention. It’s just how your body feels. It’s just Tuesday.
This is what chronic tension looks like when it’s been there long enough that you’ve stopped noticing it as a problem.
And for most women between 15 and 30 right now, it has been there long enough.
Here’s what’s actually happening.
The average person now spends over 7 hours a day looking at screens. For students and people who work at desks, it’s more. Every centimetre your head tilts forward from neutral adds approximately 4–5kg of effective load on the cervical spine, which means that the gentle forward lean most of us hold while reading a phone or laptop is placing the equivalent weight of a bowling ball on structures designed for a head held upright. Research on “tech neck” has found measurable degenerative changes in the cervical spines of people in their 20s — a finding that used to appear almost exclusively in much older adults.
That’s before stress enters the picture.
When your nervous system perceives threat; a deadline, a difficult conversation, financial anxiety, the low-level ambient stress that is just the texture of being young right now — it activates the same fight-or-flight response your ancestors used to survive predators. Cortisol and adrenaline flood the system. Muscles brace. The trapezius, the levator scapulae, the muscles along the back of the neck — they contract in preparation for a physical threat that never comes. The threat passes or doesn’t pass, but the muscle tension frequently remains, held in tissue that never fully received the signal to release.
Do this every day for months or years, and the tension stops being episodic. It becomes your resting state. Your nervous system recalibrates around it. You stop noticing it, not because it’s gone, but because it’s become background noise.
The thing nobody tells you about chronic neck and shoulder tension is that it’s not just uncomfortable. It’s expensive, physiologically. Sustained muscle contraction restricts blood flow to the tissue, which reduces oxygen delivery and allows metabolic waste to accumulate — one of the main mechanisms behind tension headaches, which affect roughly 1 in 3 people and are the most common neurological complaint in the world. Chronic tension in the upper trapezius and suboccipital muscles refers pain directly into the skull, the temples, behind the eyes, which is why so many headaches that get treated as headaches are actually neck problems in disguise.
It also feeds back into the stress system. Physical pain activates the same threat-response pathways that created the tension in the first place. The shoulders stay raised. The jaw tightens. The breath gets shallower, and shallow breathing directly elevates cortisol and keeps the sympathetic nervous system activated, which keeps the muscles contracted, which keeps the pain present.
The cycle runs quietly, underneath everything, all day.
I started looking into this because I realised I couldn’t remember the last time my shoulders weren’t tight. Not after a bad day — just consistently, as a baseline. And when I started asking around, I found that almost every woman I know in her 20s describes the same thing. The neck that never fully loosens. The shoulders that live somewhere near the ears. The headache that shows up reliably at the same time every afternoon.
We’ve accepted it as normal. It isn’t.
What I found in the research is that this is one of the most addressable physical complaints there is, not with painkillers, not with expensive treatments, but with a combination of postural awareness, specific movement, nervous system regulation, and some genuinely evidence-backed natural approaches that most people have never tried because nobody explained why they work.
This Short Dive covers all of it:
The tightness you’ve normalised is not just how your body is. It’s your body responding to something — consistently, loudly, in the only language it has.
Time to listen to it properly.
PS: We also have a subscriber-only group chat where members discuss the deep dives, share their sleep journeys, and ask me questions directly. See you there.
Disclaimer: The information and opinions expressed above are current as of the date of this post and are subject to change without notice. Materials referenced above are provided for educational and informational purposes only. None of the above constitutes medical advice, a diagnosis, a treatment recommendation, or a substitute for consultation with a qualified healthcare professional. Always seek the guidance of your doctor or another qualified health provider with any questions you may have regarding a medical condition or sleep disorder.
Short Dive below ↓
Table Of Contents:
CHAPTER 1: Why This Part of Your Body Holds Everything
The anatomy behind the tension, and why your neck and shoulders are basically stress magnets.
The neck and shoulders form a closely interconnected musculoskeletal complex that supports your head and allows a wide range of motion. This region includes the cervical spine (neck vertebrae), the shoulder joints, and many muscles that attach the head, neck, shoulder blades, and upper back. Understanding the basic anatomy will help clarify why tension often concentrates here.
Key structures of the neck and shoulders
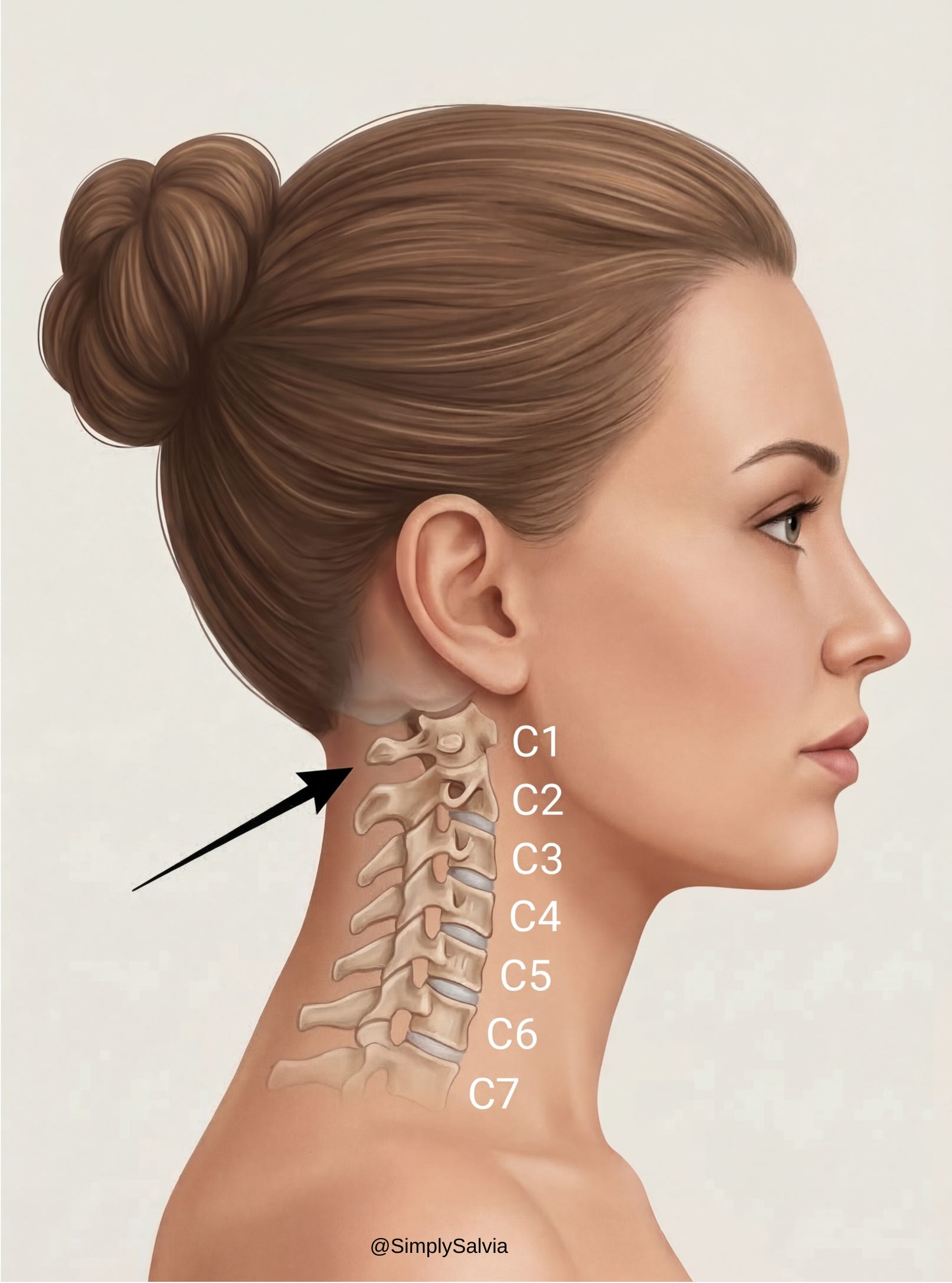
The cervical spine consists of seven small vertebrae (C1–C7) stacked between the skull and upper back. These bones protect the spinal cord and serve as attachment points for muscles. At the top, the skull sits on the atlas (C1) and axis (C2) vertebrae, enabling you to nod and rotate your head. Below, the lower cervical vertebrae connect down to the thoracic spine of your upper back. The shoulders are built around the scapulae (shoulder blades) and clavicles (collarbones), which articulate with the upper arm bones. A key joint is where the clavicle meets the scapula (at the acromion) this, along with muscles, secures the shoulder girdle to the neck and thorax.
The Muscles You Keep Hearing About And What They Actually Do
Several big muscle groups span the neck and shoulder region, and these are often the source (and victim) of tension:
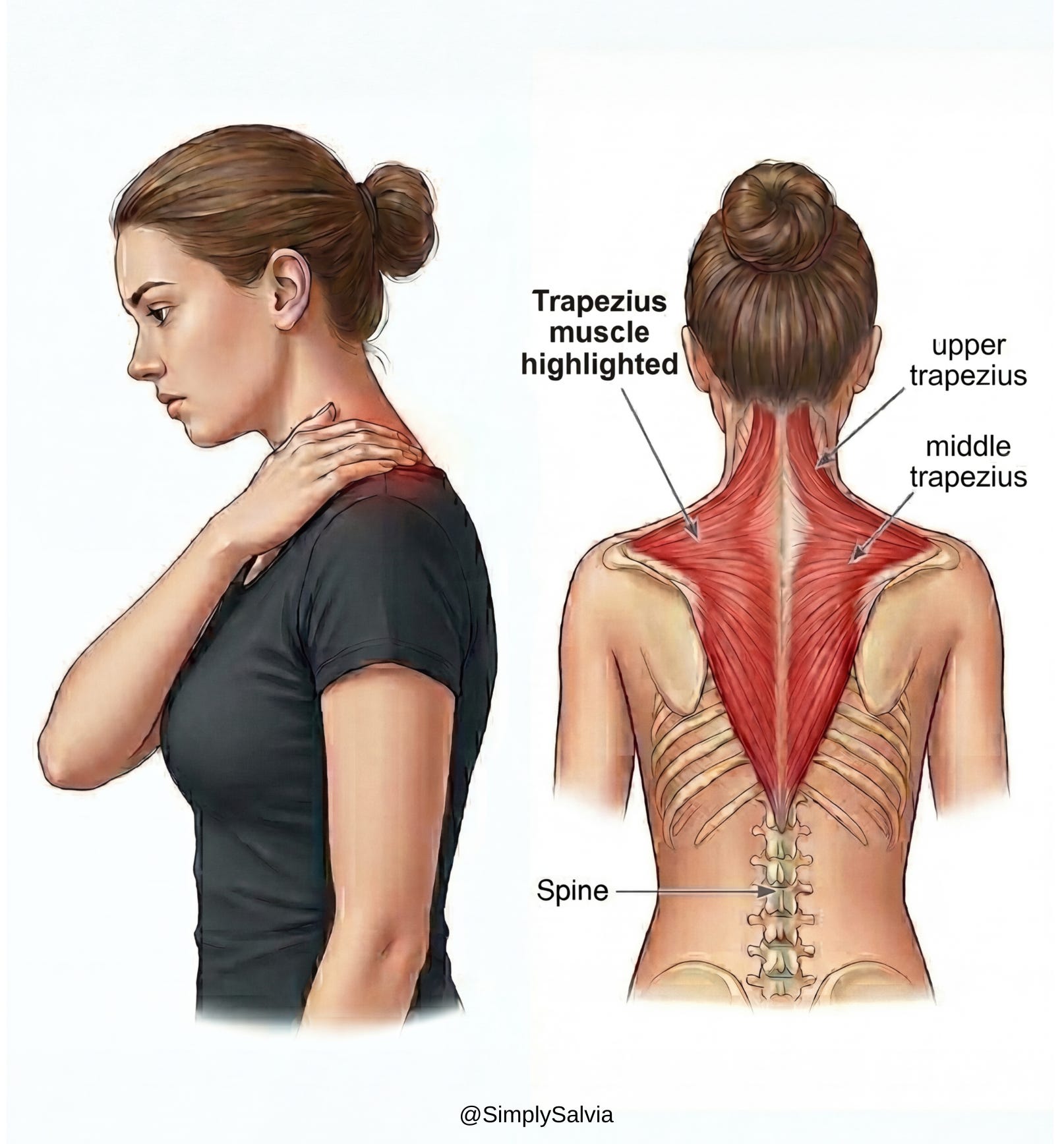
Trapezius muscles (upper back/neck)
The trapezius is a large kite-shaped muscle on each side of your upper back, running from the base of the skull across the shoulders and down to mid-back. The upper trapezius fibers are the ones you feel tightening when you shrug. They help support your head, stabilize the shoulder blades, and assist in neck/shoulder movement. The trapezius is so commonly tight under stress that it’s nicknamed the “stress muscle,” as it tends to hold lots of tension during times of anxiety or prolonged sitting. If you’ve ever felt hard knots or soreness at the tops of your shoulders, your traps are complaining!
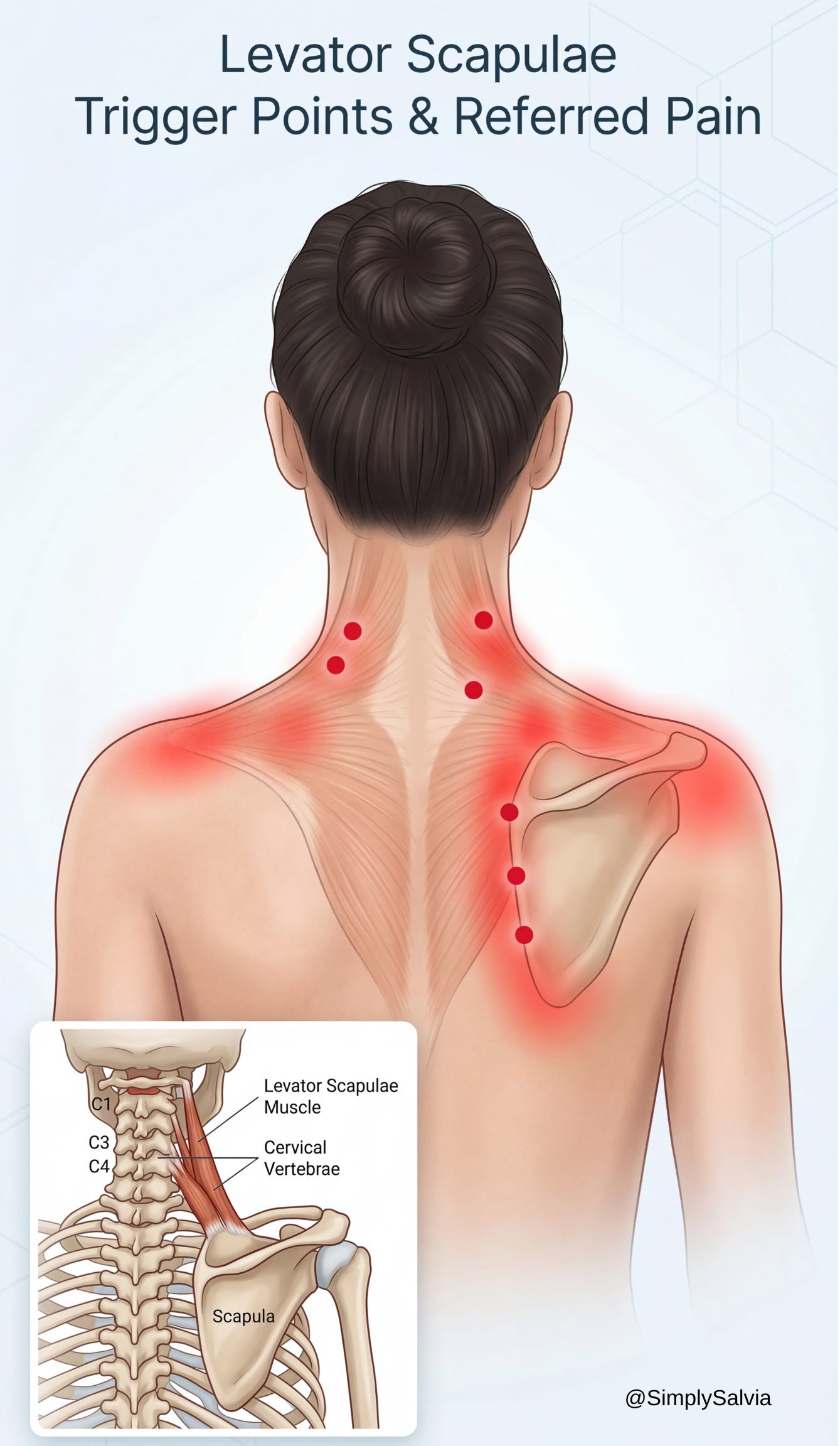
Levator scapulae (side of neck)
This pair of strap-like muscles runs from the cervical vertebrae down to the top of the shoulder blades. As the name suggests, their job is to “elevate the scapulae,” i.e. lift your shoulder blades (like when you shrug). They also assist in neck extension and rotation. The levator scapulae often become overstressed with forward head posture, when your head juts forward, these muscles must strain to hold the head up and stabilize the shoulders. Tight levators are a common culprit in a stiff neck and can even refer pain into the head, contributing to tension-type headaches.
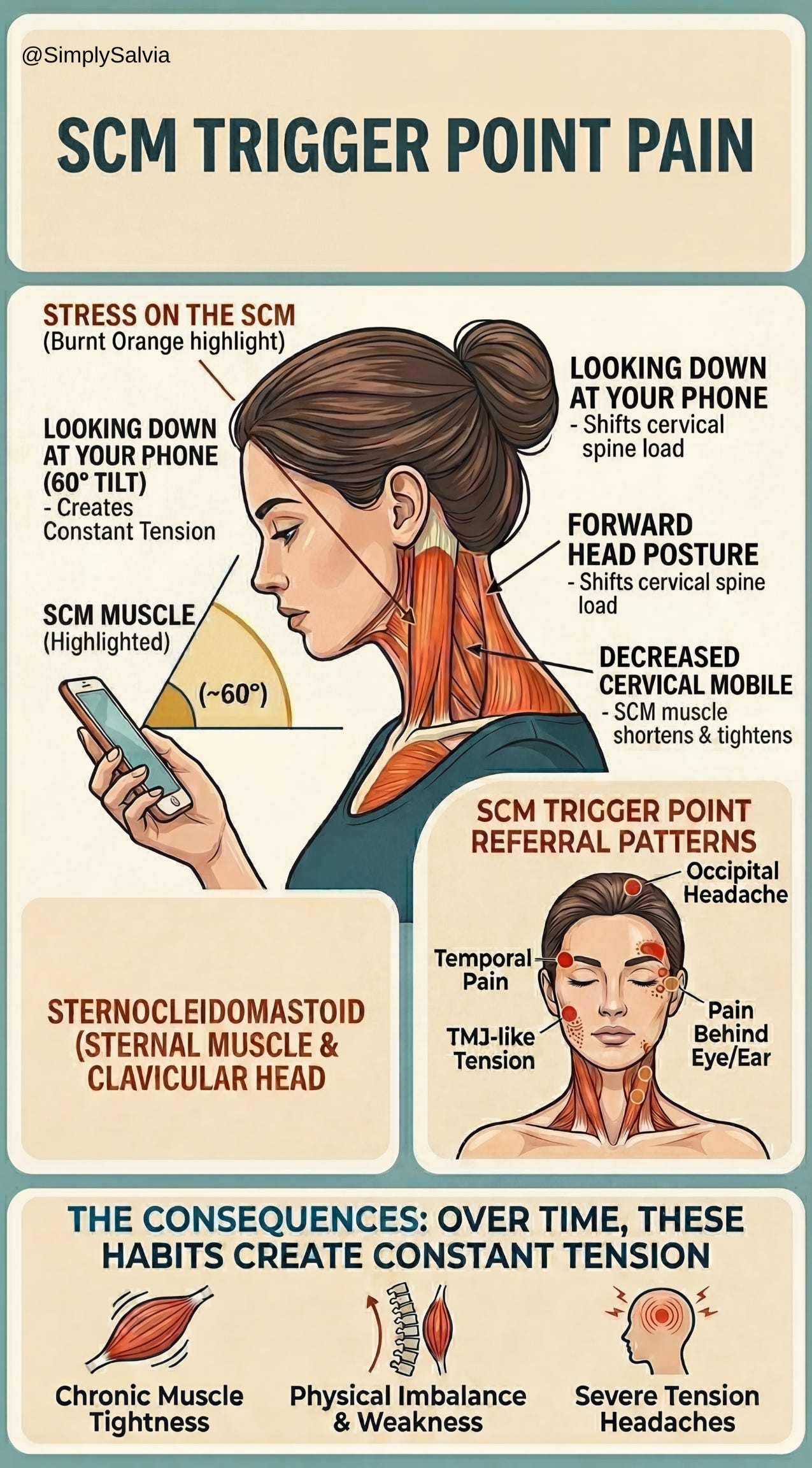
Sternocleidomastoid (SCM, front/side of neck)
The SCM is the prominent rope-like muscle that runs diagonally from behind your ear (mastoid bone) down to your collarbone and sternum in the front of your neck. You can usually see or feel it pop out when you turn your head to the side. The SCM’s actions include rotating and tilting the head, and it helps stabilize the head on the spine. It’s one of the most active neck muscles and can become tight from things like constantly looking down or poor head posture. Chronic SCM tension or trigger points may cause pain that radiates to the head, jaw, or even behind the eyes. (Notably, poor posture and even habits like sleeping on too high a pillow or on your stomach can aggravate the SCM, I’ll revisit this in causes.)
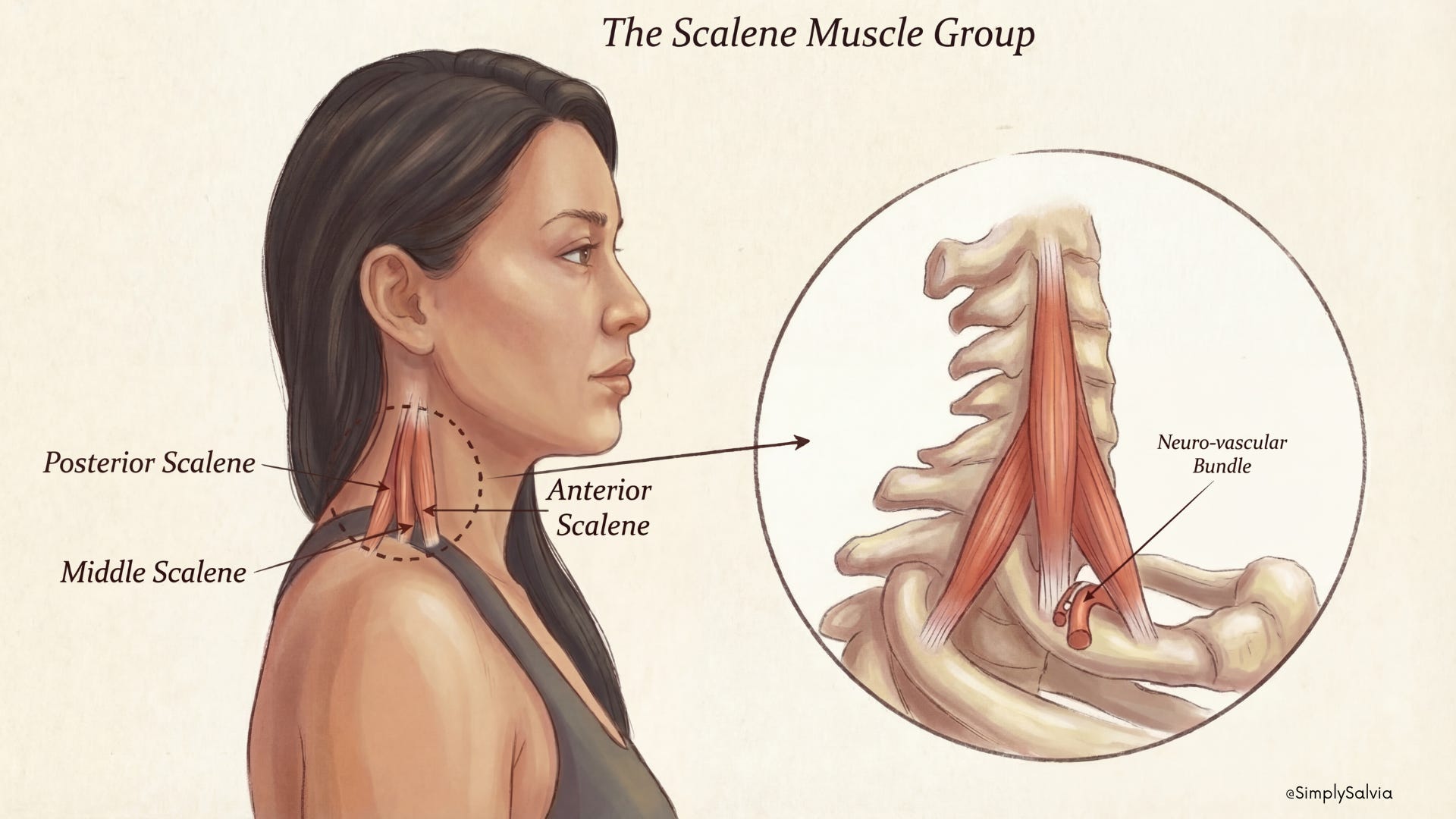
Scalenes (deep side of neck)
The anterior, middle, and posterior scalenes are three smaller muscles situated deeper in the side of the neck. They run from the cervical vertebrae to the first two ribs. The scalenes help bend the neck sideways and assist with breathing (lifting the ribs during inhalation). These can get overworked especially in people who breathe shallowly or who have forward-head posture. Tight scalenes can also compress nerves and blood vessels that run through the neck area (contributing to conditions like thoracic outlet syndrome, discussed later).
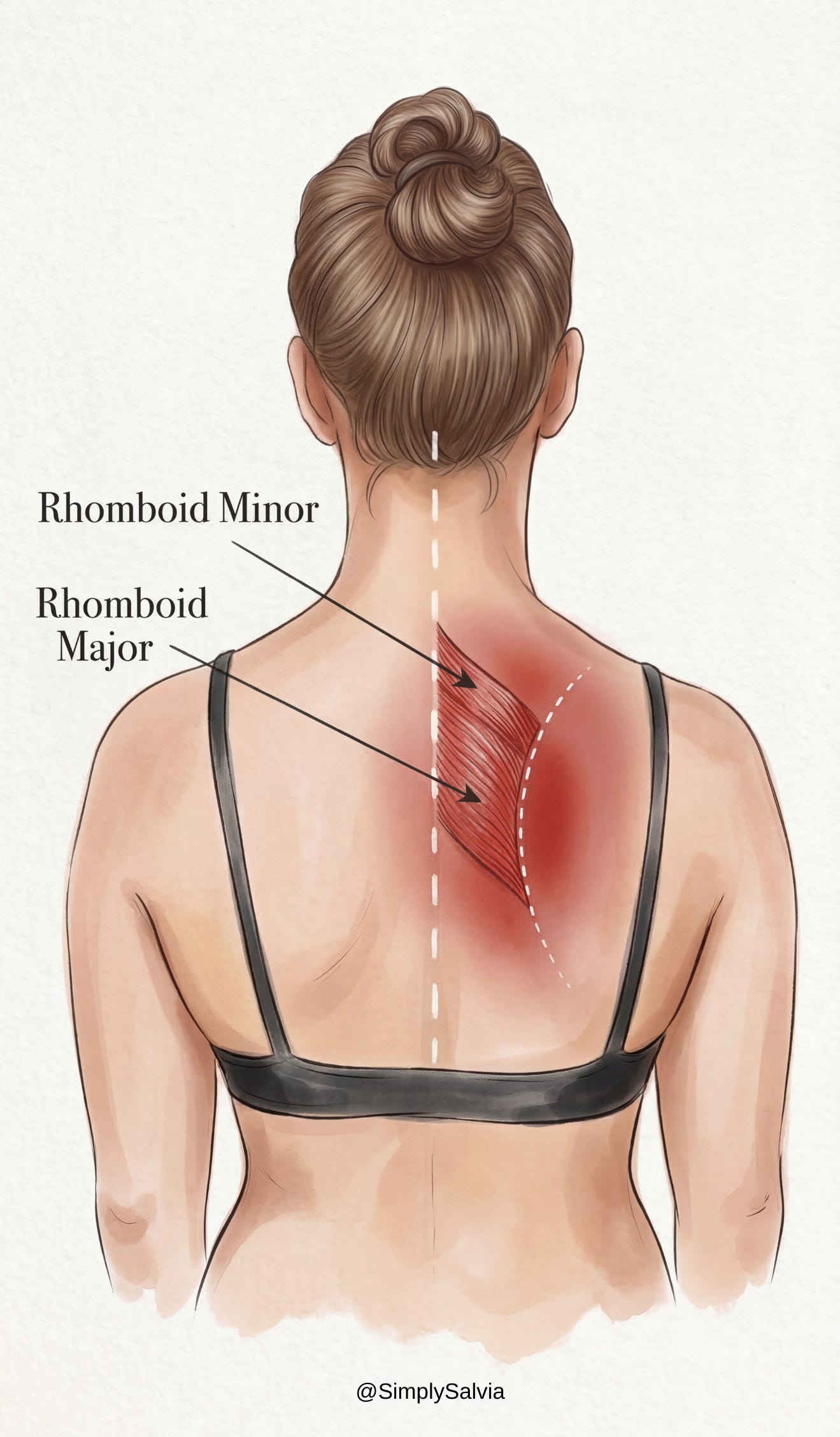
Rhomboids (upper back)
The rhomboid major and minor are upper-back muscles connecting the inner edges of your shoulder blades to the spine (around the upper thoracic vertebrae). Their job is to retract and stabilize the shoulder blades, basically pulling your shoulders back and together. They form part of the postural support for your shoulders. If you slouch or round your shoulders forward a lot, the rhomboids get stretched out and weakened, which can lead to upper back strain and knots between the shoulder blades. Conversely, sometimes they spasm from trying to constantly yank the shoulder blades back into alignment. If you’ve ever felt burning pain between your shoulder blades after a long day at the computer, thank your rhomboids.
These muscles (along with others like the upper spinal extensors, pectoral chest muscles, and small suboccipital muscles at the base of the skull) work together to hold up your 10–12 pound head and coordinate the intricate movements of your head, neck, and shoulders. When they’re balanced and conditioned, you maintain good posture and pain-free movement. But under stress or strain, they can easily become dysregulated.
How things work (or break down)
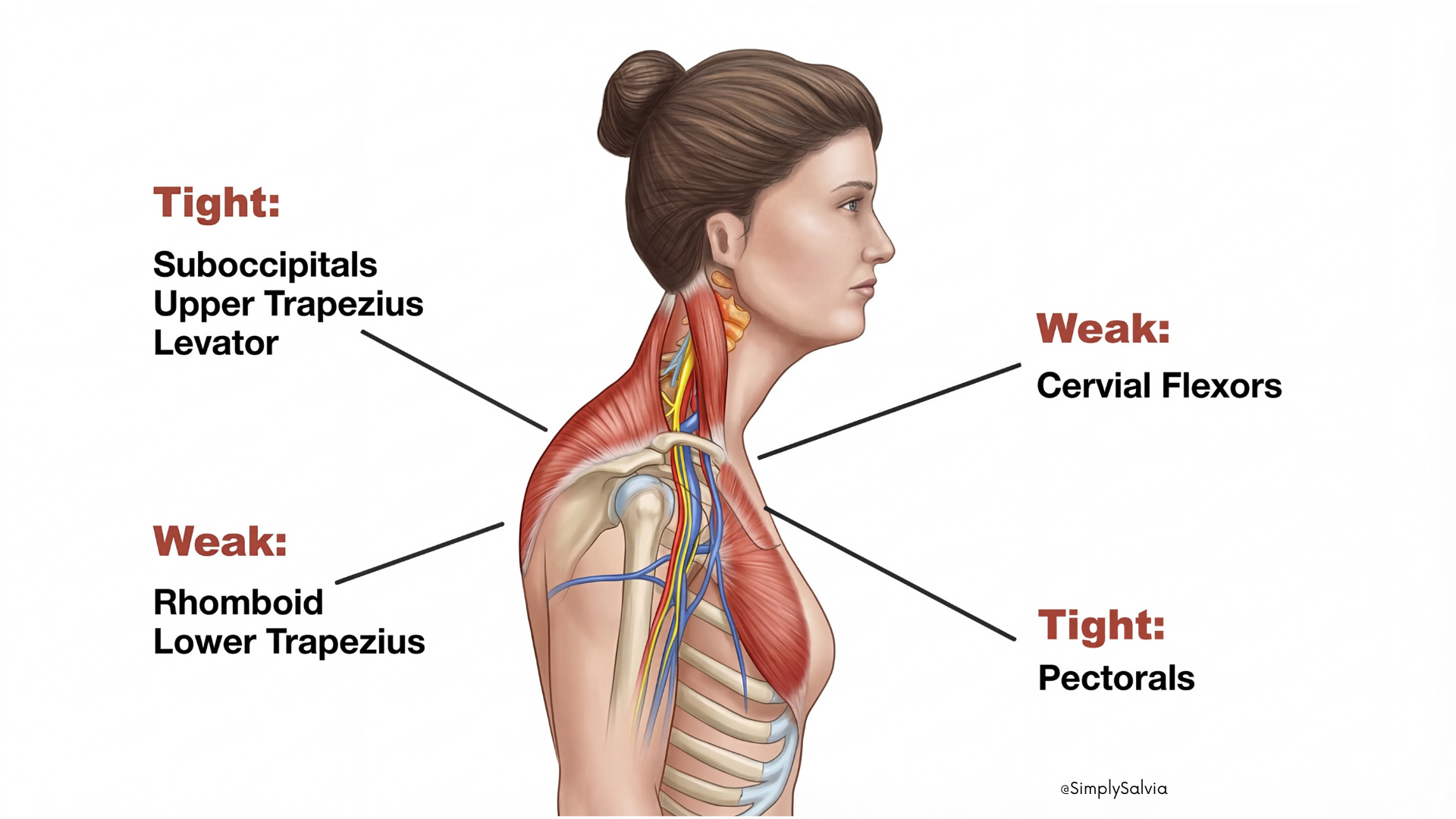
In an ideal scenario, your head sits directly over your shoulders with ears aligned roughly over them. Your trapezius and levator scapulae hold the shoulder blades in a neutral position. The neck muscles in front (SCM) and back (extensors) balance each other to keep your head upright. The smaller stabilizers (scalenes, deep neck flexors) fine tune movements. Problems arise when this balance is disturbed for example, by a forward head posture, rounded shoulders, or prolonged static positions. Muscles like the trapezius and levator scapulae then have to work overtime (often in a fixed, contracted state), leading to fatigue and pain. This is exacerbated by stress, which causes certain muscles to contract involuntarily (a subconscious bracing response). Over time, tight muscle bands and “knots” (myofascial trigger points) can form in these areas, further restricting movement and causing discomfort.
To sum up, the neck/shoulder complex is a sophisticated system that unfortunately easily falls victim to the demands of modern life. A basic grasp of these anatomy points will help make sense of the causes of tension I discuss next, and why specific remedies (like posture correction or targeted stretches) can make a difference.
CHAPTER 2: What’s Actually Causing Your Tension
It’s almost never just one thing. Here’s what’s really behind it.
In this chapter, I’ll explore common causes of neck and shoulder tension many of which will likely sound familiar as well as some less obvious contributors that people often overlook. Usually, it’s not just one factor, but a combination of physical and psychological stresses that tighten up our neck and shoulders. By identifying your personal triggers, you can start making changes to prevent tension before it starts.
The Obvious Causes
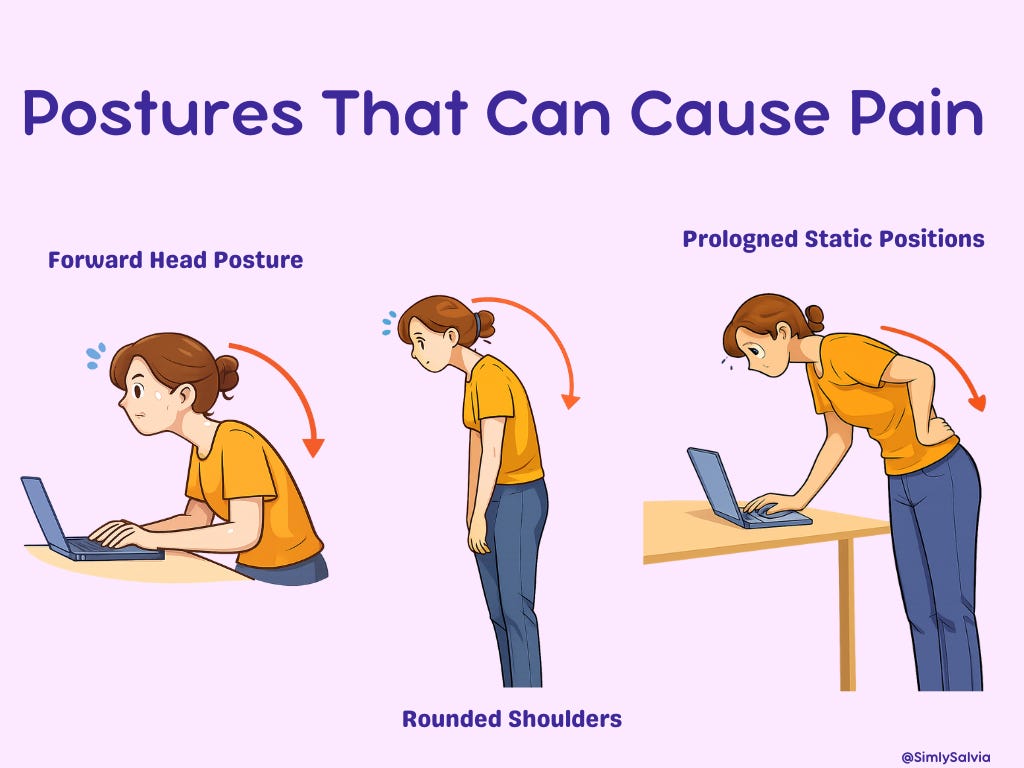
Forward Head Posture and Screen Habits
Arguably the number 1 cause of chronic neck/shoulder tightness is the way we sit, stand, and position our bodies during daily activities. In today’s world, many of us spend hours with a forward head posture, think of leaning your head out toward a computer screen or downward at a phone. This so-called “text neck” significantly increases strain on the neck. Biomechanically, for every inch your head juts forward, the effective weight load on your neck doubles or more. One landmark analysis showed that a head tilted 60° forward exerts about 60 pounds of force on the neck, compared to roughly 10–12 pounds in a neutral upright position. It’s easy to see how slumping over a screen for long periods can fatigue the neck and upper back muscles!
Poor workstation ergonomics such as a low monitor, non-supportive chair, or keyboard/mouse positioned too far away also encourage slouching and shoulder rounding. This leads to overstretched, weak upper back muscles and chronically contracted chest and shoulder muscles (classic “upper crossed syndrome” posture). Over time, poor alignment causes muscle imbalances and persistent tension. Even outside the office, daily habits like cradling a phone between your ear and shoulder or always looking downward while walking can contribute. The result of long-term poor posture is a stiff, achy neck and often tension headaches. As one physiotherapy resource plainly states:
Forward head posture increases compressive load on the cervical spine and leads to muscle tension, pain, and headaches.
Stress and Anxiety
Psychological stress is a major driver of muscular tension in the neck/shoulder region. When you’re under stress whether due to work deadlines, exams, personal conflicts, or general anxiety, your body tends to engage in muscle guarding. Essentially, the neck and shoulder muscles involuntarily contract as part of the stress response (as if your body is subconsciously bracing for a threat). Mental stress triggers tightening of the neck and shoulder muscles, often without you realizing it until pain sets in. Think of the idioms “shouldering responsibilities” or something being a “pain in the neck” they exist for a reason! People who are anxious or stressed commonly report a feeling of the shoulders being “up to the ears” or a constant tight band across the upper back. This tension is often accompanied by shallow breathing (which itself can overuse neck muscles like the scalenes) and elevated cortisol levels, which may heighten pain perception. Over time, chronic stress can sensitize muscles and nerves, leading to myofascial trigger points that maintain tension even at rest. I’ll discuss relaxation techniques in Chapter 6 to counter this cause.
Overuse or Repetitive Strain
Your neck and shoulders can also become tight from physical overuse – that is, repeatedly engaging the same muscles in strenuous activity without adequate rest. Athletes and manual laborers are prime examples: a swimmer doing countless freestyle strokes, a weightlifter doing heavy shrugs, or a construction worker lifting overhead repeatedly. These motions can cause small micro-tears in muscle fibers and lead to inflammation, causing the muscles to tighten up protectively. Certain occupations and hobbies put particular strain on the neck/shoulder complex. For instance, musicians can develop neck and shoulder tension, violinists and violists often hold an instrument clamped under the chin leading to neck muscle strain, while flutists frequently report left neck and shoulder pain due to holding their arms up and head turned. Even something like driving all day or carrying a heavy backpack can count as repetitive strain. Overuse initially causes acute soreness, but if one continues the activity without sufficient recovery, the muscles adapt by becoming chronically tight and shortened. In some cases, the strain isn’t muscular but tendinous for example, rotator cuff tendinitis or biceps tendon strain can cause referred pain and guarding in the shoulder region. Previous injuries or trauma can also lead to long term tension: after something like a whiplash (neck injury commonly from car accidents) or a shoulder sprain, the affected muscles often go into spasm and may remain tight for weeks or months during the healing process. Without proper rehab, some people are left with chronic neck stiffness after a whiplash injury.
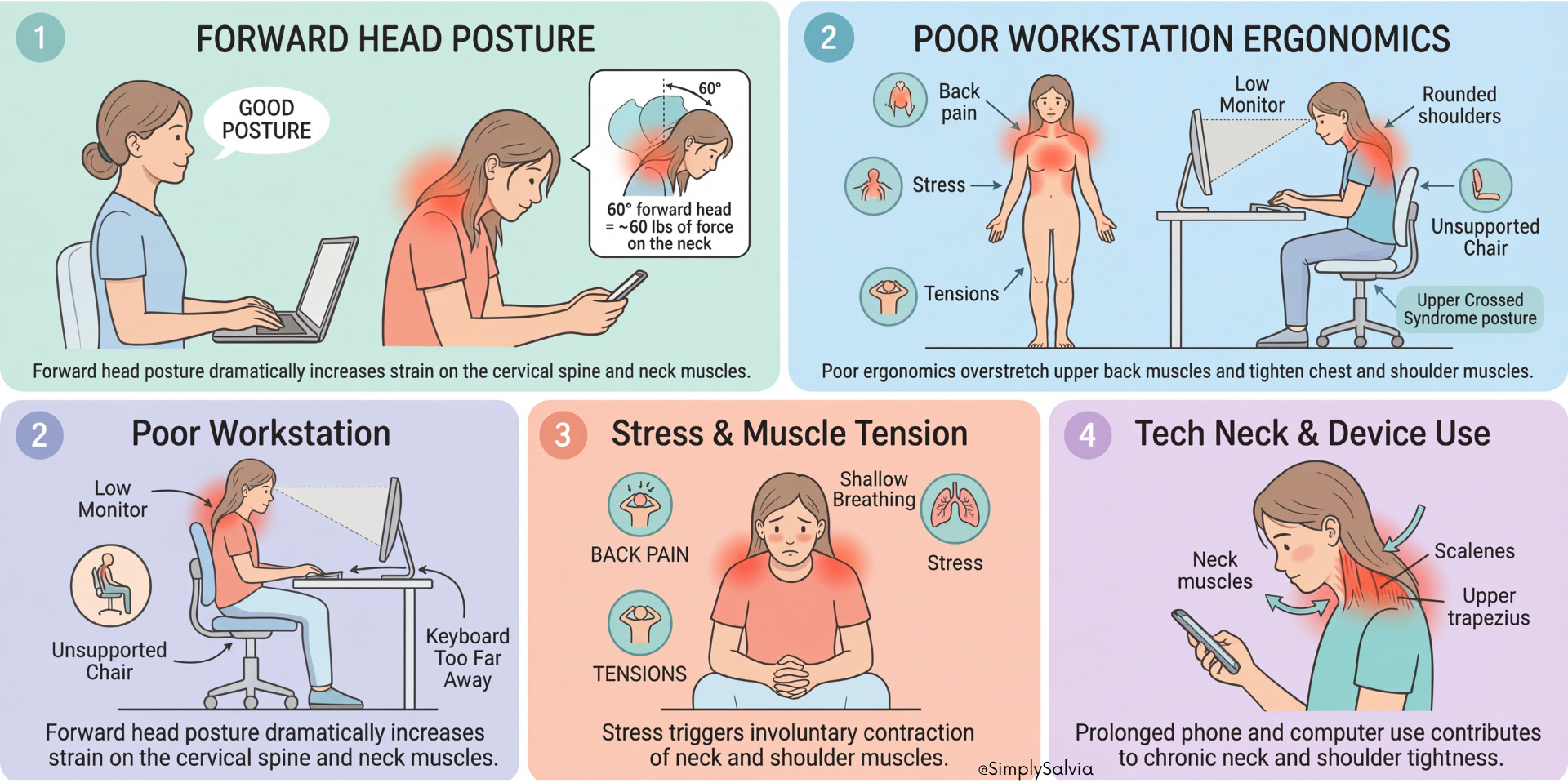
“Tech neck” and Device Use
While this overlaps with poor posture, it’s worth singling out our excessive use of phones, tablets, and computers. Constantly looking down at a smartphone (often called text neck) puts the neck in a flexed position for prolonged periods. Likewise, hours of typing or gaming can cause you to hunch forward. The result is a one-two punch of forward head and rounded shoulders, which fatigues neck extensors and tightens chest/shoulder muscles. It’s not just adults; teens and college students often report neck/shoulder pain linked to screen time. Despite the name, “tech neck” is not just a buzzword research shows that sustained forward head posture from device use correlates with increased neck pain in young populations. On the flip side, there’s evidence that correcting posture and taking frequent breaks from screens can significantly reduce this pain (more on prevention in Chapter 6). The bottom line is that our modern tech-heavy lifestyle literally shapes our musculoskeletal health.
The Less Obvious Causes (That Most People Miss)
Poor sleep position
How you sleep can greatly affect your neck and shoulder muscles. Using an unsupportive pillow or sleeping in a twisted position may strain the neck for hours at night. For example, sleeping with a pillow that’s too high can force your neck into an extreme side-bent position; too flat and your head may flop backward. Perhaps the worst habit is stomach sleeping, which requires you to rotate your head sharply to one side and often jam an arm under the pillow, this can tighten neck joints and muscles and put pressure on shoulders. It’s no surprise people often wake up with a crick in the neck or numbness from a bad sleep posture. In fact, clinicians note that inappropriate pillow height or sleeping on the stomach can precipitate sternocleidomastoid and neck muscle issues. Ideally, your pillow should keep your head neutral (as if standing with good posture) and avoid prolonged end-range neck rotation or bending.
Jaw tension and teeth grinding (bruxism)
The jaw and neck are intricately connected via muscular and nerve pathways. If you clench your jaw frequently during the day or grind your teeth at night (a condition called bruxism), you may also be tensing up your neck without realizing it. Jaw clenching engages muscles like the temporalis and masseter, but studies have shown it also co-activates some neck muscles during sleep bruxism. Ever wake up with a sore jaw and tight neck? That’s a telltale sign. Bruxism can trigger tension and stiffness in the neck and shoulder muscles as well as headaches. Similarly, temporomandibular joint (TMJ) disorders – problems with the jaw joint often refer pain to the neck and upper back. Patients with TMJ dysfunction commonly report neck and shoulder pain alongside jaw pain. So, that habitual jaw clenching while stressed, or grinding at night, could be contributing to your stiff neck. Managing bruxism (through night guards, relaxation, or dental intervention) can in turn relieve some neck/shoulder tension.
Carrying heavy bags or loads on one side
Do you often lug a heavy purse, tote, or backpack on the same shoulder? Or perhaps you’re a parent who carries a toddler on one hip regularly? These habits can create muscle imbalances and strain. Chronically carrying a heavy bag on one side causes you to elevate that shoulder and lean to one side, leading to neck and shoulder pain. The trapezius and levator scapulae on that side become overworked from supporting the weight, while the spine and opposite side muscles may compensate. Over time, this can cause one shoulder to sit higher than the other and lead to tightness and soreness that is persistently worse on the side of the load. The term “rucksack palsy” even exists for nerve irritation from backpack straps. To prevent this, lighten your load when possible and alternate sides or use a backpack that distributes weight evenly. When carrying a child on the hip, be conscious of switching sides frequently (and consider a supportive carrier that straps to both shoulders).

Vision problems/eyestrain
Believe it or not, your eyesight can affect your neck posture. If you have uncorrected vision issues or even simple eye strain, you might unconsciously jut your head forward or tilt it to see better, straining your neck over time. For instance, someone with progressive lenses might tilt their head back to look through a certain part of their glasses, or someone nearsighted might lean in toward a screen. This chronic head-forward or tilted positioning can tighten neck extensors and lead to muscle imbalances. Optometrists note that poor vision alignment can cause the brain to strain eye muscles and “tilt the head,” putting extra work on the neck. If you find yourself craning your neck to read or constantly looking down because your monitor is too low, your vision or setup might be contributing to your pain. Regular eye exams and ergonomic adjustments (like raising your screen to eye level) can help mitigate this factor.
Dehydration and electrolyte imbalance
Even mild dehydration can make muscles more prone to cramping and tightness. Our muscle cells need adequate water and electrolytes (like magnesium, potassium, calcium) to contract and relax properly. If you’re not drinking enough fluids or you sweat a lot without replenishing, your neck and shoulder muscles might be more likely to spasm or feel stiff due to poor hydration status. Research shows that dehydration increases the chances of muscle stiffness and soreness. Low levels of electrolytes especially magnesium are known to cause muscle fibers to stay tense (more on nutritional factors in Chapter 5). Thus, something as simple as not drinking enough water or an imbalance in minerals could exacerbate your tension. Many people notice more neck/shoulder cramping during hot weather or after long workdays with too much coffee and not enough water. The fix: keep hydrated and consider electrolyte-rich foods or drinks if you suspect this is an issue.
Sedentary lifestyle & muscle deconditioning
Lastly, a lack of movement can be as problematic as overuse. If you sit most of the day and rarely exercise the muscles of your upper body, those muscles can become weak and easily fatigued, contributing to poor posture and strain. The neck and upper back rely on endurance of postural muscles to hold the head upright; if these muscles are deconditioned, the extra load of your head can cause tightness (as the body recruits whatever it can to prevent the head from flopping forward). A sedentary lifestyle also means more hours in static positions (often poor ones) which, as I covered, causes stiffness. The phrase “motion is lotion” applies here, without regular movement and stretching, connective tissues can shorten and muscles become less pliable. The end result is that even mild tasks, like carrying groceries or sleeping in an odd position, can trigger neck or shoulder pain because the tissues aren’t resilient. This cause is fixable by gradually introducing strengthening and mobility exercises (I’ll cover those in Chapter 6). It’s encouraging to know that improving fitness can directly reduce musculoskeletal pain.
As you can see, neck and shoulder tension usually has multifactorial origins. Most commonly, it’s a combination: for example, a stressed individual with a desk job (stress + poor posture + sedentary), or an athlete who also has anxiety (overuse + stress). Identifying the causes relevant to you is important as it might be as straightforward as adjusting your monitor height and taking stretch breaks, or as complex as managing stress and changing how you sleep. In all cases, a holistic approach (addressing both the physical and mental contributors) works best for relief.
Before I jump into solutions, however, I need to touch on something critical: not all neck/shoulder pain is “just tension.” It’s important to know when these symptoms could signal a more serious underlying condition.
CHAPTER 3: When to Take It More Seriously
Most neck tension is benign, but here’s how to know when it isn’t.
Not all neck and shoulder pain originates from simple muscle tension or lifestyle factors. Sometimes, persistent or severe pain in these areas can be a sign of an underlying medical condition. In this chapter, I’ll briefly review some conditions that can present with neck and shoulder symptoms, so you know what warning signs to watch for. The goal isn’t to make you worry, but rather to empower you to distinguish a benign muscle strain from something that might require medical evaluation. I’ll also outline “red flag” symptoms that indicate you should seek professional help sooner rather than later.
Conditions That Can Look Like ‘Just Tension’
Cervical osteoarthritis (cervical spondylosis): This is essentially wear and tear arthritis of the neck, a very common condition, especially as we age. With time, the discs between neck vertebrae dry out and shrink, and the joints develop arthritis and bone spurs. In fact, over 85% of people older than 60 show signs of cervical spondylosis on imaging (though not all have symptoms). When symptomatic, cervical arthritis can cause chronic neck stiffness, aching in the neck/shoulders, and sometimes nerve pain if bone spurs pinch nearby nerves. You might feel or hear grinding/popping (crepitus) when turning your neck. Morning stiffness that improves throughout the day is common. Spondylosis can also contribute to tension headaches. The good news is that in most cases it’s manageable with conservative care (exercise, physical therapy, etc.), but it’s useful to recognize that chronic neck ache and reduced range of motion especially in older people could be arthritic in nature rather than just muscular.
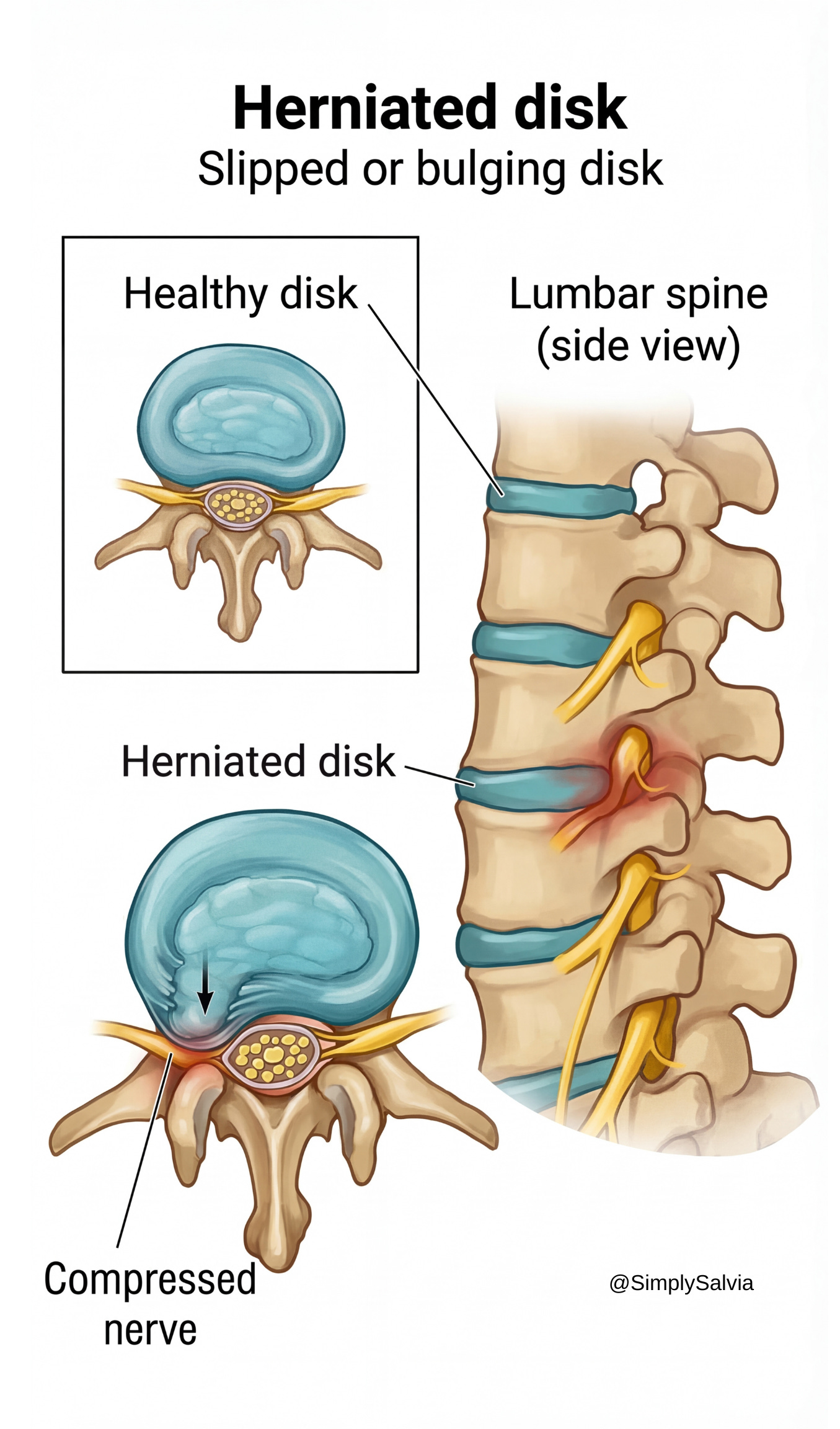
Cervical disc herniation or nerve impingement: A herniated disc in the neck occurs when the soft gel-like center of a cervical disc protrudes through a tear in the outer layer, potentially pressing on spinal nerves. This can happen from injury or degeneration. A herniated disc in the C5–C7 region, for example, might compress a nerve root that innervates the shoulder, arm, or scapular region. Symptoms can include neck pain with sharp, radiating pain or tingling down one shoulder/arm (radiculopathy), as well as muscle weakness in the arm or hand. In some cases, people describe a deep ache between the shoulder blades or in the shoulder itself, which is actually referred nerve pain. A pinched nerve in the neck (from a disc or arthritic narrowing) is often distinguishable by this radiating pattern and neurological signs like numbness or reflex changes. If you experience these symptoms, it’s more than just muscle tension and you’d want to see a doctor. That said, muscular tension and pinched nerves can be interrelated: a tight muscle can irritate a nerve, and nerve pain can cause muscles to spasm. Many of the common causes I listed (poor posture, etc.) over time can contribute to disc problems.
Key warning sign: pain, numbness, or burning sensations radiating down the arm or into the hand, especially if accompanied by weakness, should be evaluated. (Mechanical neck pain from tension generally stays local to the neck/shoulder and doesn’t cause true numbness or significant weakness.)
Thoracic outlet syndrome (TOS): This is a condition where the nerves or blood vessels that pass through the lower neck into the arm (the brachial plexus and subclavian vessels) get compressed, often between tight muscles or an extra rib. TOS can cause a variety of symptoms including neck and shoulder pain, along with arm symptoms like numbness or swelling. It’s somewhat uncommon but can be misdiagnosed as general neck/shoulder strain. For example, someone might have chronic shoulder aching and tingling in the fingers due to nerve compression by a tight scalene muscle or an anomalous rib. Thoracic outlet syndrome pain often feels like a dull ache in the neck, shoulder, or upper chest that may worsen when raising the arms. If you have tension plus weird arm symptoms (pins and needles, circulation changes), TOS is one possibility. Repetitive overhead motions (like pitching or swimming) can predispose someone to TOS, as can injuries like whiplash. Treatments often involve physical therapy to open up the outlet.
The main point: TOS involves more than just muscle pain, it includes nerve/vascular symptoms so it’s something to be aware of if your shoulder/neck tension is accompanied by arm issues.
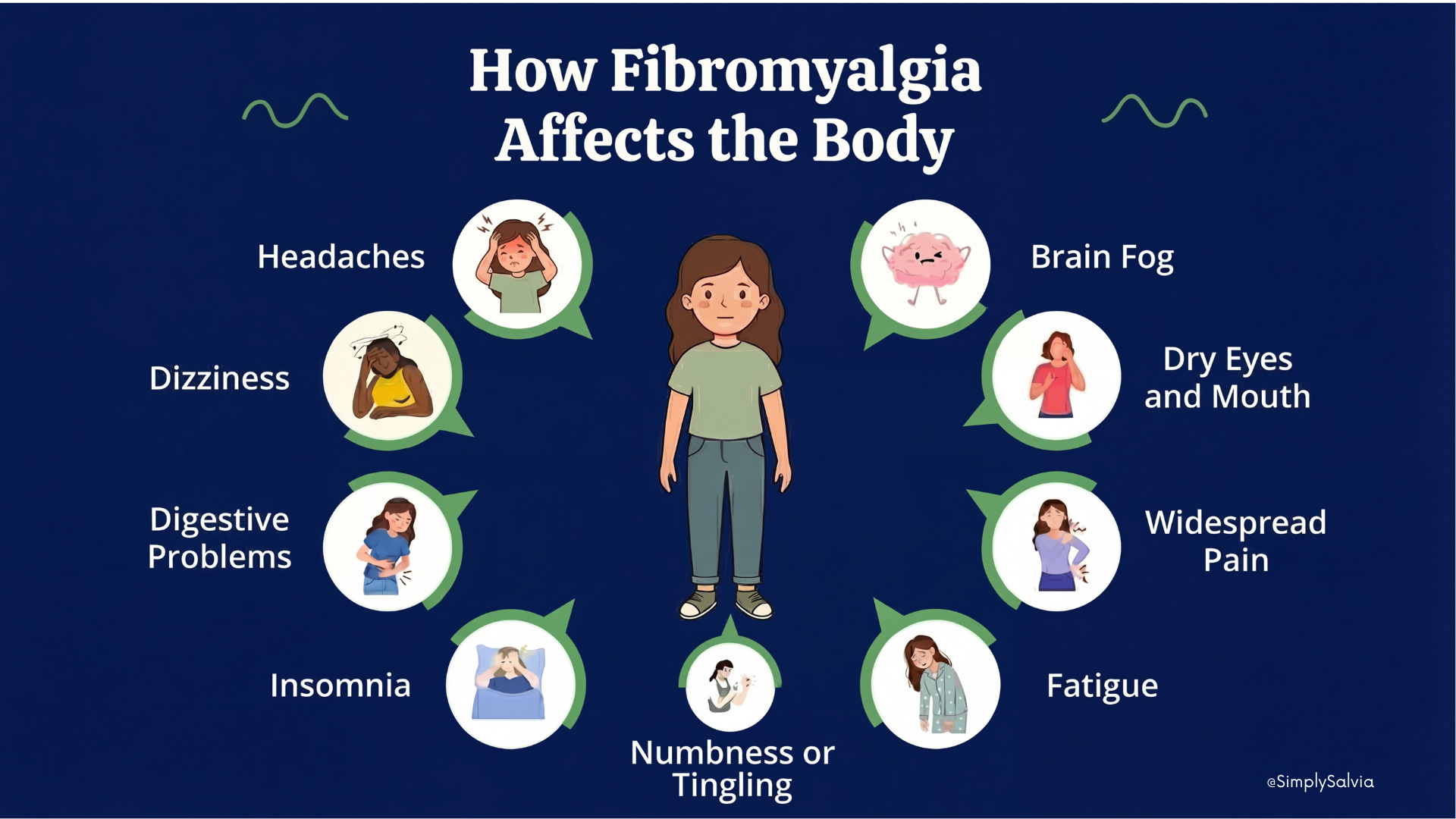
Fibromyalgia: Fibromyalgia is a chronic pain syndrome characterized by widespread musculoskeletal pain, fatigue, and tender points. The neck and shoulders are notorious sites of pain in fibromyalgia. In fact, pain often starts in one area such as the neck and shoulders and then generalizes. People with fibromyalgia frequently experience extreme muscle tenderness in the shoulder girdle and neck, which can feel like persistent tension but is actually part of a broader central pain processing issue. If your neck and shoulder pain is accompanied by symptoms like generalized body aches, poor sleep, “brain fog,” and multiple tender points, fibromyalgia could be a consideration. Of course, muscle tension from fibromyalgia will still benefit from many of the natural strategies I’ll discuss (exercise, stress reduction), but fibromyalgia is a more complex systemic condition. Importantly, fibromyalgia is a diagnosis of exclusion, doctors would rule out other causes (like hypothyroidism or autoimmune disease) if widespread pain is present.
Polymyalgia rheumatica (PMR): This is an inflammatory condition usually affecting older adults (over 50, often over 70). It causes severe pain and stiffness in the shoulders and neck (and often the hips). Someone with PMR often has intense stiffness in the neck/shoulders, especially in the morning, that improves throughout the day. The pain can be bilateral and is often accompanied by fatigue or mild fever. It’s caused by systemic inflammation and is closely associated with another condition, giant cell arteritis. The key is that PMR causes muscle pain and stiffness in the neck/shoulder girdle that is pretty dramatic, and it typically responds rapidly to low-dose corticosteroids. If you are in the right age group and have sudden onset of shoulder/neck girdle pain and morning stiffness, PMR is a possibility and definitely something a doctor should evaluate, as it’s easily treatable and important to catch (especially because of the arteritis risk).
Temporomandibular joint (TMJ) disorder: I touched on this in causes with jaw tension. TMJ disorders (problems with the jaw joint and chewing muscles) can present not just with jaw pain or clicking, but also neck and upper shoulder pain. The muscles of the jaw (mastication muscles) have connections to cervical muscles. It’s actually common for patients with TMJ dysfunction to report neck stiffness and pain between the shoulder blades. If your neck/shoulder tension comes along with jaw pain, popping or locking of the jaw, or clenching habits, treating the TMJ issue can be key to relief.
Tension-type headaches or migraines: Chronic headaches can both result from and contribute to neck/shoulder tension. Tension headaches often feature a band of pain around the head and tightness in the neck and scalp muscles. The neck is actually a trigger zone, muscle tension in the neck and base of the skull can provoke headaches, which is why massage or heat on the neck often helps relieve a tension headache. Migraines, too, sometimes present with neck pain (some migraine sufferers feel neck stiffness before or after an attack). If you have frequent headaches with your shoulder tension, it could be a two-way street: the headaches could be causing you to tense up, and your tense muscles could be making headaches more likely. Addressing the muscle tension can improve headache frequency. Conversely, if you treat the headaches, the muscle tension may ease. Pay attention to headache “red flags” though like if a headache is accompanied by fever, neurological changes, or is sudden and severe (“thunderclap”), seek medical care.

Cardiac referred pain (angina): It’s worth noting that sometimes pain in the left shoulder, left neck, or between the shoulder blades can be a referred pain from the heart, especially in cases of angina or heart attack. Women in particular may experience heart attack symptoms as pain in the neck, jaw, or shoulder blades rather than the classic chest pain. The pain of angina (due to heart not getting enough oxygen) can radiate to those areas because of how the nerves converge in the spinal cord. Typically, this pain comes on with exertion and may be accompanied by other symptoms like shortness of breath, sweating, or chest pressure. Angina from a heart issue is often felt in the left side of the neck or shoulder (or arm) rather than only the chest. If your left-sided neck/shoulder pain is associated with exertion or other cardiac symptoms, it should be evaluated urgently. It goes without saying: any sudden or severe neck/shoulder pain that feels different from a muscle ache, especially if you have risk factors, warrants caution to rule out cardiac causes. (This is rare, so don’t panic but be aware.)
In addition to the specific conditions above, there are others like thoracic spine issues, osteoporosis-related fractures, spinal cord injuries, infections (like meningitis or a spinal abscess), or even certain cancers that can manifest as neck or shoulder pain. These are uncommon in the grand scheme, but it’s important to be aware of warning signs that your pain is not the garden-variety muscle tension.
Red Flags — See a Doctor If You Have Any of These
So, how do you tell if your neck/shoulder tension is just muscular or something more? Here are some red flags that merit a medical evaluation:
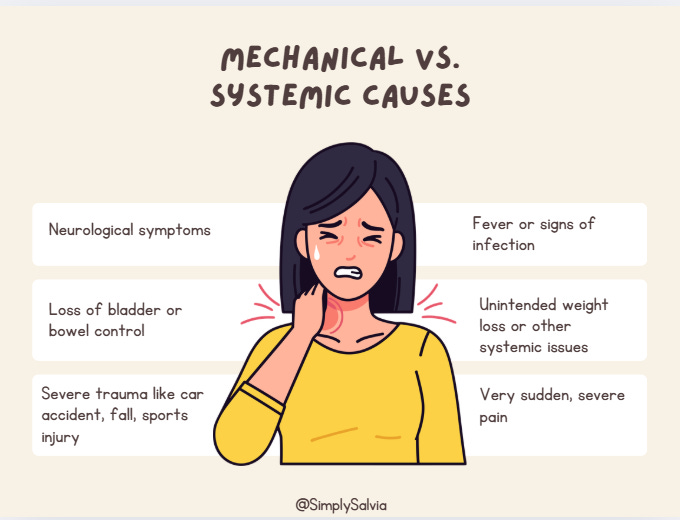
Neurological symptoms: If you experience numbness, tingling, or weakness in your arms or hands alongside the neck/shoulder pain, it could indicate nerve involvement (e.g. a herniated disc pinching a nerve, or something affecting the spinal cord). For example, if you have trouble lifting your arm or notice your hand dexterity is off, that’s not normal muscle tightness. Seek care if pain is accompanied by radiating tingling or weakness in the limbs.
Loss of bladder or bowel control: This is rare, but if neck problems progress to where you have any loss of control over bladder/bowels, it could signal severe spinal cord compression. This is a medical emergency. (Typically seen in very severe cervical spine issues or injuries).
Severe trauma: If your pain began after a significant injury, say a car accident (whiplash), a fall, or sports collision you should get it checked. Sudden onset after trauma could mean fractures or tissue damage that needs proper treatment. Even if it seems “just muscular,” ruling out something like a small fracture or torn ligament is important. Also, pain that persists no matter what position (even at rest) after an accident is a warning sign.
Fever or signs of infection: If you have neck stiffness plus fever, chills, or unexplained fatigue, it could indicate something like meningitis (infection of the meninges around the brain/spinal cord) or another infection. A stiff neck with fever and headache is a classic meningitis sign and needs immediate medical attention. Other infection signs could include swollen lymph nodes, sore throat (if it’s something like mono causing neck pain), or recent infections that spread to soft tissues. While muscle tension alone won’t cause a fever, an infection can absolutely cause neck stiffness (the muscles become rigid). Don’t ignore these systemic symptoms.
Unintended weight loss or other systemic issues: Chronic neck pain accompanied by weight loss, night sweats, or generally feeling unwell might point to something more systemic (like an autoimmune condition or even a tumor). For instance, apical lung tumors (Pancoast tumors) can cause shoulder/neck pain by invading nerves though again, very rare. Unexplained weight loss or constant pain that doesn’t change with movement is a red flag.
Very sudden, severe pain: If you experience the worst neck pain of your life that comes on suddenly, consider getting evaluated. While muscle strains can hurt a lot, a sudden severe neck pain could be something like an arterial dissection in the neck or another acute issue. This is more about erring on the side of caution. Gradual onset pain associated with activity is more typical for benign causes.
No improvement with normal remedies: If you’ve tried rest, heat, stretching, etc., and the pain never eases up even a little after a week or so, that’s a clue it might not be typical muscle tension. Most simple strains start to slowly improve with conservative care. Persistent, unchanging pain should be checked out.
To be clear, most neck and shoulder tension is not due to ominous causes, and you don’t need to run to the doctor for every twinge. But it’s wise to recognize these warning signs. If in doubt, especially if neurological or systemic red flags are present, see a healthcare provider. They may do an exam, and if needed, imaging (X-ray, MRI) or blood tests to rule out specific conditions.
Now that I’ve covered that important context, let’s assume you’re dealing with garden-variety neck/shoulder tension (the common scenario). The next chapter will discuss how not all tension is the same, meaning, there are different types of muscle tightness and pain patterns. Understanding the type of tension you have can further guide the best relief strategies.
CHAPTER 4: Not All Tension Is the Same
Understanding what type you have changes how you treat it.
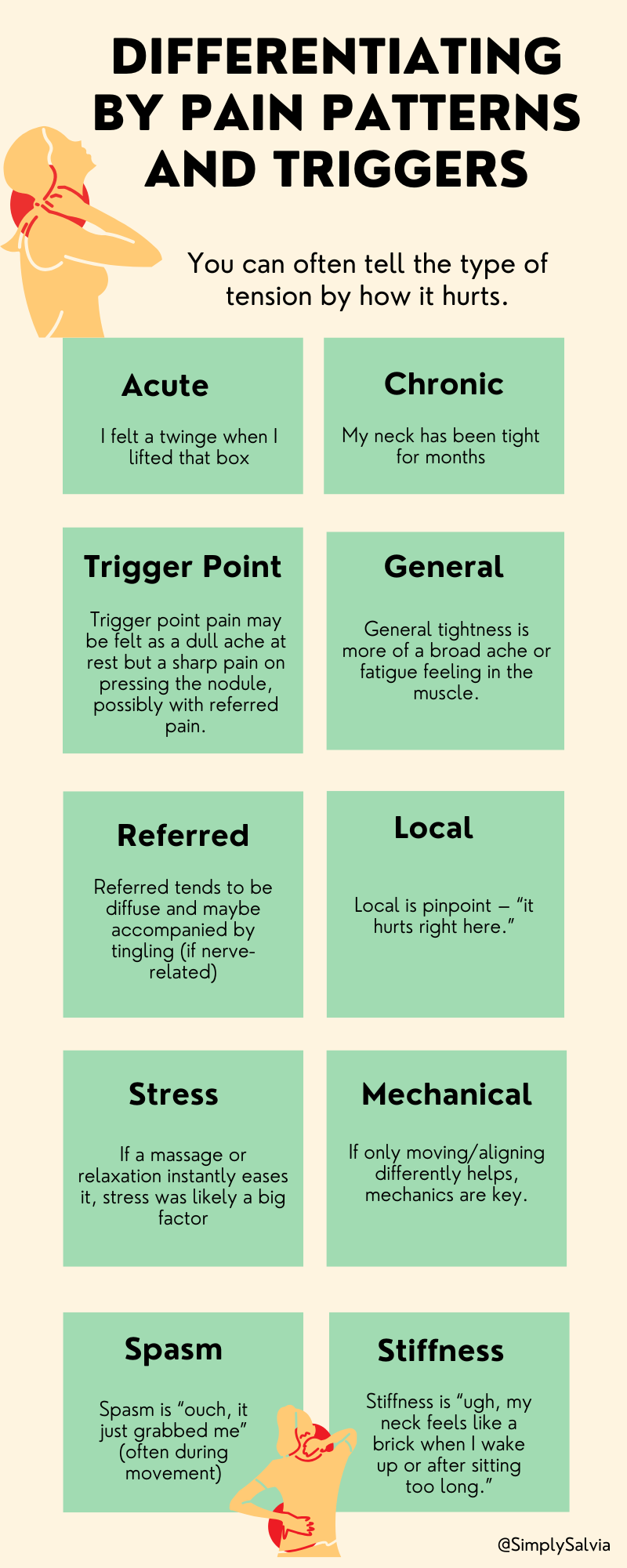
If you’ve ever wondered why one person’s neck tightness comes with sharp “knots” and trigger points, while another has a dull, constant ache, or why your own pain can vary from a stiff feeling to sudden spasms know it’s because not all muscle tension is created equal. In this chapter, I’ll differentiate several types of neck and shoulder tension. Recognizing what type (or combination) you’re experiencing can help you target the right treatment. I’ll look at acute vs. chronic tension, myofascial trigger points vs. general muscle tightness, referred vs. localized pain, stress-related vs. mechanical tension, and muscle spasms vs. stiffness.
Acute vs. chronic tension
Acute tension is short-term muscle tightness that comes on quickly, often in response to a specific event or stressor. For example, you might wake up with a crick in your neck from sleeping funny, or your shoulders might bunch up during a stressful meeting but then relax afterward. Acute tension often involves the muscle contracting as a protective reflex (like after a minor strain or injury) or due to sudden stress, and it typically resolves in days to a few weeks.
Chronic tension, on the other hand, is long-lasting tightness that persists for months or more. This is the kind many office workers or stressed individuals know well. It is the feeling that your neck and shoulders are perpetually tight or knotted. Chronic tension can lead to muscle fibrosis (thickening) and adaptive shortening of muscles. It often waxes and wanes but never fully goes away. Acute tension is usually easier to relieve (with rest, heat, a massage, etc.), whereas chronic tension might require more consistent lifestyle changes and therapy to undo, as the muscles have essentially learned to stay in a guarded state.
Myofascial trigger points vs. general muscle tightness
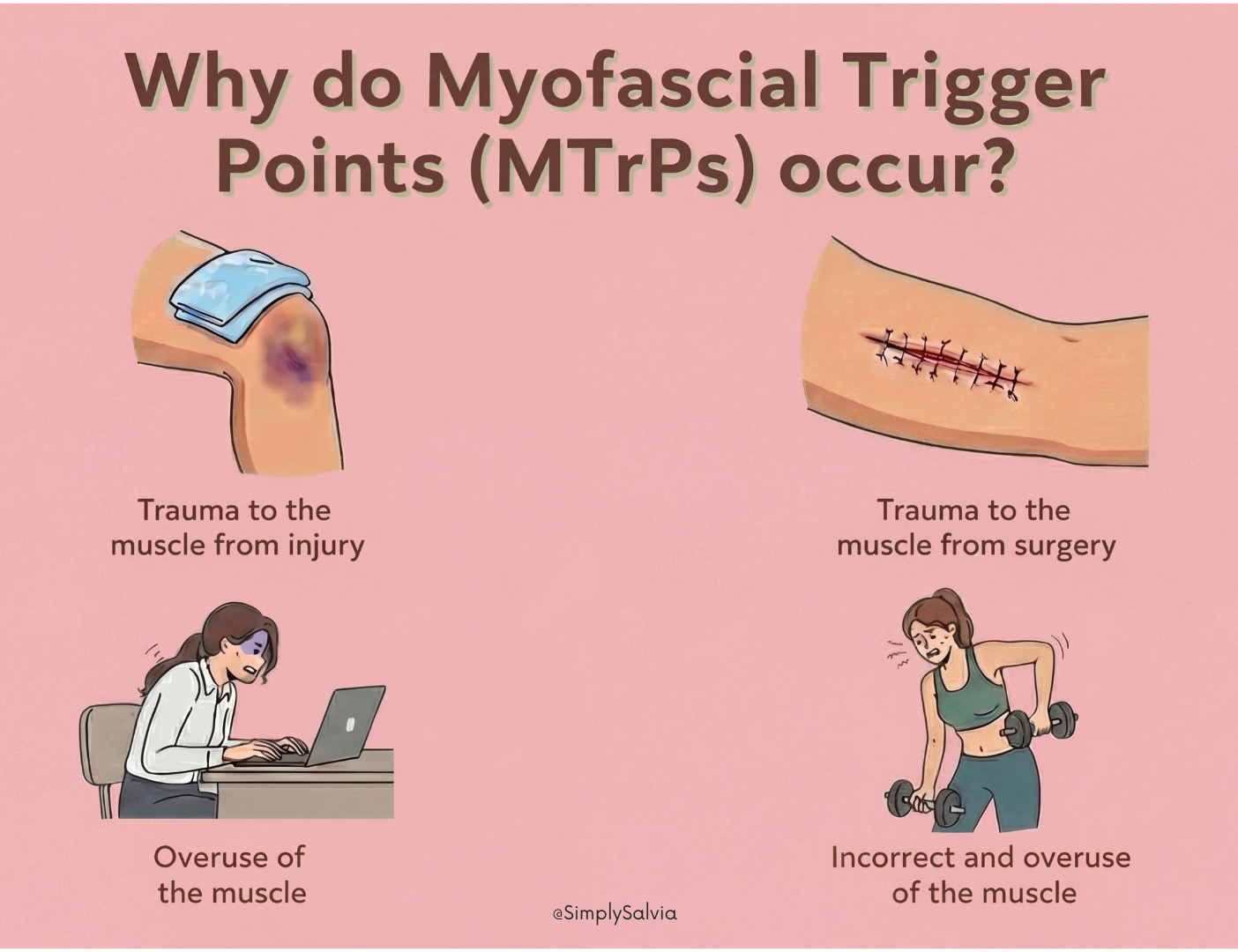
Have you ever pressed on a tender “knot” in your neck muscle that sent pain shooting to another area? That was likely a myofascial trigger point. A trigger point is essentially a hyper-irritable spot in a tight band of muscle fiber, a small patch of muscle that is stuck in contraction. Pressing on it can be quite painful and may produce referred pain in a predictable pattern (for example, a trigger point in the upper trapezius might refer pain upward into the skull or behind the eye). Trigger points feel like little nodules or tight lumps in the muscle and cause pain when touched (and sometimes even when not touched).
In contrast, general muscle tightness is more diffuse, the muscle is overall tense, but there isn’t necessarily a specific knot you can pinpoint. General tightness might feel like a broad stiffness or firmness in the muscle without focal tenderness. Trigger points are often a result of chronic overload of specific fibers and can be stubborn; they might require targeted treatment like trigger point massage, needling, or specific stretches to release. General tightness responds well to global approaches like heat and whole-muscle stretching. It’s common to have both: a generally tight muscle that also contains some active trigger points. For example, someone’s whole upper trapezius might be tight, but they have a few zinger spots near the top of the shoulders that are especially bad – those are trigger points. When dealing with trigger points, techniques like sustained pressure (ischemic compression) or rolling on a ball can help release them. For general tightness, relaxing the muscle through stretching or heat might suffice. Recognizing if you have trigger points can validate why your pain sometimes radiates, it’s not “in your head,” it’s a myofascial phenomenon.
Referred pain vs. local pain
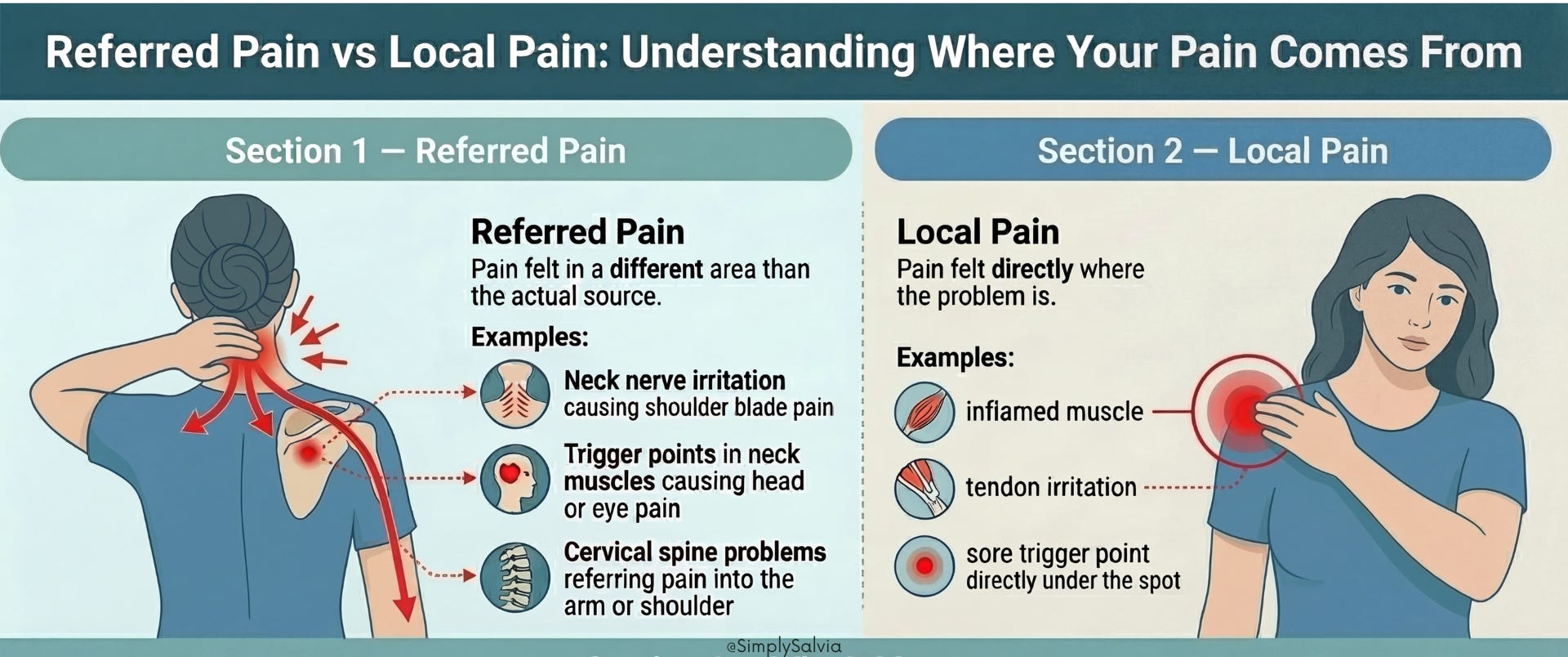
Referred pain means the sensation of pain is felt in a location different from the actual source. In neck and shoulder issues, referred pain is pretty common. For instance, a problem in your neck joints or nerves might refer pain into the shoulder blade or down the arm. Trigger points, as mentioned, can also refer pain e.g., a trigger point in a neck muscle causes eye or head pain.
Local pain is felt directly where the issue is like a sore spot in the shoulder that hurts right there when you press it. Understanding if some of your pain is referred can prevent chasing the wrong problem. A classic example: some people think they have a shoulder problem because their shoulder blade area hurts, but it’s actually referred from the neck (like a C5-C6 nerve impingement). Conversely, a sore spot on top of the shoulder that hurts only there is likely local (perhaps an inflamed muscle or tendon at that site). As discussed in the last chapter, even heart or gallbladder issues can refer pain to the shoulder region though those usually have other clues. In a musculoskeletal sense, note where your pain travels. Does pressing your neck reproduce your shoulder pain? That could mean the neck is the source. Does massaging a spot in your upper back send pain elsewhere? That’s a trigger point referring. Treating the underlying source (be it a neck issue or a trigger point) will then alleviate the referred pain.
Stress-related vs. biomechanical tension
It’s useful to tease out whether your muscle tension is primarily driven by psycho-emotional factors or physical/mechanical ones. Stress-related tension tends to fluctuate with your mental state for example, your neck tightness might flare up on particularly hectic days or during anxiety, even if your posture and activity level didn’t change. This type often comes with symptoms like tension headaches, clenched jaw, or shallow breathing when stressed. Techniques like deep breathing, meditation, or a hot bath (which calms the nervous system) may dramatically reduce this tension.
On the other hand, biomechanical tension is more related to how you move (or don’t move) and your body positions. It might get worse after a long day of sitting or after you perform a certain repetitive motion. It’s less influenced by mood and more by physical factors (posture, ergonomics, strength). Of course, the two often overlap, stress can make you sit poorly or hold your body rigidly, combining both elements. But identifying the primary driver can guide your focus. If you realize, “Whenever I’m anxious, my shoulders bunch up,” then stress management is key. If you realize, “My neck is fine on weekends but kills me after a day at the computer,” then ergonomic and movement fixes are key. Often, both need addressing (like adjusting your workstation and doing relaxation exercises). In upcoming chapters, I’ll cover both mind-body and physical interventions for precisely this reason.
Muscle spasms vs. stiffness
These terms are sometimes used interchangeably, but they have different connotations. A muscle spasm is a sudden, involuntary contraction of a muscle. It can be quite painful (a charley horse is a classic spasm, though usually in the calf). In the neck or shoulders, a spasm might feel like the muscle “locked up” suddenly. For example, you turn your head quickly and a neck muscle seizes, that’s an acute spasm. Spasms are often short-lived (seconds to minutes), though residual soreness can last a while. They can be caused by acute strain, fatigue, dehydration, or abrupt movements.
Muscle stiffness, in contrast, is more of a continuous feeling of tightness or reduced flexibility. Stiffness is that feeling when you wake up and your neck is hard to turn not necessarily from a momentary cramp, but from a persistent tightness. If someone says “I have a stiff neck,” they usually mean they can move it, but with difficulty and discomfort (not that it’s violently contracting by itself).
Why distinguish these? Because a spasm might respond well to things like gentle stretching after it releases, or magnesium supplementation if due to electrolyte issues, whereas chronic stiffness might respond better to heat and slow mobilization. If you have frequent spasms (acute cramps) in your neck/shoulders, you’d look for different triggers (like dehydration or specific motions) compared to chronic stiffness (where you’d consider posture and chronic inflammation). Also, note that what people call a “muscle knot” is not exactly a spasm it’s more of a localized tight spot (trigger point) that causes a stiff, dull pain. A spasm is usually sharper and more sudden.
By understanding these differences, you can tailor your approach. For instance, if you identify trigger points, you’ll spend time with a lacrosse ball or seek a massage therapist who can do trigger point release. If you realize your pain is mostly stress-related tension, you might prioritize daily breathing exercises and meditation. If it’s chronic stiffness, perhaps daily stretches and posture work are in order. Of course, many people have a mix (e.g., chronic stiffness with some trigger points, plus an occasional spasm when they overdo it). In practice, you’ll likely apply multiple strategies and in the next chapters, I’ll equip you with those. But having this nuanced view of tension types ensures you use the right tools for the job.
Before moving on to remedies, also consider whether nutritional factors might be playing a role in your muscle tension. Sometimes, what’s going on inside your body (vitamin/mineral levels, hydration, diet-induced inflammation) can influence how tight or prone to pain your muscles are. That’s up next.
You now know why.
Why the neck and shoulders carry everything — the anatomy, the layered muscles, the way this region sits at the intersection of your skeletal load and your nervous system’s threat response. Why the tension keeps coming back even when you’ve had a massage or slept well for a week. Why not all tightness is the same, and why treating postural tension the same way you’d treat stress-held tension will get you nowhere. And when the ache stops being something to manage yourself.
That understanding is the part most people skip. They go straight to the foam roller, the hot shower, the ibuprofen, and the tension comes back, because they were treating the symptom without knowing what was driving it.
Part 2 is where it becomes practical. And specific.
Chapter 5 covers what you’re eating and drinking that may be quietly feeding the tension — the magnesium deficiency most young women don’t know they have, the caffeine and dehydration connection, the inflammatory dietary patterns that keep muscles in a heightened state.
Chapter 6 is the relief toolkit: the specific posture fixes that address tech neck at its structural source, the stretches that are actually worth doing, and the section most guides leave out; how to regulate the nervous system itself, which is the only way to release tension that’s being held there by stress rather than mechanics.
Chapter 7 covers the herbal and topical remedies with real evidence: what to drink, what to apply, and what the research actually says about each one.
Chapter 8 is the one to read if self-care has taken you as far as it can.
Plus a full daily action plan — what to do this week, what to build over the next month, and how to maintain it so the tension stops being your default setting.
The tightness you’ve normalised is not permanent. But it won’t shift on its own.
Upgrade to read Part 2 →
The information in this post is for educational and informational purposes only and does not constitute medical advice or a substitute for consultation with a qualified healthcare professional.
References:
Cleveland Clinic (2022). Neck Pain (Cervicalgia) – Overview & Causes. (Noting neck pain is common, affecting about 10–20% of adults at any time)my.clevelandclinic.orgmy.clevelandclinic.org
Verywell Mind – Wisner, W. (2025). Why You May Be Carrying Stress in Your Shoulders and Neck. (Explains that the neck and shoulders are among the most common areas for stress-related muscle tightness; stress causes muscles to tighten, leading to tension)verywellmind.comverywellmind.com
Equilibrio Massage – Trombley, N. (2023). “Do you hold stress in your neck and shoulders?” (Mentions the trapezius is often called the “stress muscle” because it holds a lot of tension when we’re anxious or sit too long)equilibriomassage.com
Physiopedia – Levator Scapulae. (Details how forward head posture increases tension in levator scapulae muscles, potentially causing neck pain and headaches)physio-pedia.com
Hansraj, K.K. (2014). Assessment of Stresses in the Cervical Spine Caused by Posture and Position of the Head. Surgical Technology International 25. (Found that a 60° forward head tilt places about 60 lbs of force on the neck vs. 10–12 lbs in neutral)pingeprii.ee
Physiopedia – Forward Head Posture. (Notes that forward head posture increases compressive loads on the neck and leads to muscle tension, neck pain, and headaches)physio-pedia.com
Physiopedia – Sternocleidomastoid Syndrome. (Lists poor posture, high pillows, stomach sleeping, anxiety, and stress as causes of SCM muscle tension and pain)physio-pedia.com
Michigan Head & Neck Institute (n.d.). Bruxism Causes – Neck Clenching. (Bruxism – teeth grinding – can cause neck stiffness and tension in neck/shoulder muscles)michiganheadandneck.com
Border Therapy Services (2020). Can Carrying a Heavy Purse Cause Shoulder Damage? (Habitually carrying a heavy bag on one side affects posture and can lead to neck, shoulder, and back pain)bordertherapy.com
Identity Physical Therapy (2022). Why Your Neck Pain Might Be a Vision Problem. (Poor vision or eye strain can lead to forward head posture as one subconsciously leans in, straining neck muscles)identitypt.com
Cleveland Clinic (2023). Muscle Stiffness – Causes & Prevention. (Research shows dehydration increases likelihood of muscle stiffness and soreness; staying hydrated and maintaining electrolyte balance is important for muscle relaxation)my.clevelandclinic.org
Mayo Clinic (n.d.). Cervical Spondylosis – Symptoms & Causes. (Age-related wear in the neck is very common; over 85% of people over 60 have cervical spondylosis, which can cause chronic neck stiffness and pain)mayoclinic.orgmayoclinic.org
Cleveland Clinic (2022). Neck Pain – Possible Causes. (Poor posture, weak abdominal muscles, and stress can all contribute to neck pain; whiplash from trauma is a common injury causing neck tension)my.clevelandclinic.orgmy.clevelandclinic.org
Cleveland Clinic (n.d.). *Thoracic Outlet Syndrome (TOS). * (TOS compresses nerves/vessels between neck and shoulder, causing pain in neck, shoulder, and arm – often a dull ache worsened by arm movement)my.clevelandclinic.orgmy.clevelandclinic.org
Johns Hopkins Medicine (n.d.). Fibromyalgia. (Fibromyalgia often presents with pain starting in neck and shoulders; widespread musculoskeletal pain can include chronic neck/shoulder tension)hopkinsmedicine.org
National Institute of Arthritis (NIAMS) (2016). Polymyalgia Rheumatica Info. (PMR causes inflammatory pain and stiffness chiefly in shoulders, neck, and hips – often severe in mornings)niams.nih.gov
Macon TMJ & Sleep Center (n.d.). Neck and Shoulder Pain in TMD. (Temporomandibular disorder frequently leads to neck and shoulder pain; patients with TMJ issues commonly have associated neck muscle tension)tmjsleepmacon.com
Cleveland Clinic (2020). Tension Headache – Causes. (Muscle tension in neck and scalp is believed to trigger tension-type headaches; prolonged poor posture or stress tightening these muscles is a major factor)my.clevelandclinic.org
Wikipedia (2020). Referred Pain. (Explains angina from heart attack often refers pain to left neck and shoulder rather than chest)en.wikipedia.org
Cleveland Clinic (2022). Neck Pain – When to Seek Care. (Urgent medical care is advised if neck pain follows trauma, or if accompanied by fever, significant headache, numbness/tingling in arms, or weakness – signs of possible serious issues like meningitis or nerve compression)my.clevelandclinic.orgmy.clevelandclinic.org
Cleveland Clinic (2023). Myofascial Pain Syndrome. (Trigger points are small muscle “knots” that cause pain locally and in referred patterns; relieving trigger points is key in treating chronic muscle tension)my.clevelandclinic.org
Salt Laboratory (n.d.). Magnesium for Muscle Cramps & Stiffness. (Magnesium is crucial for muscle relaxation; low levels can lead to muscle tightness and cramping)saltlaboratory.com
The Permanente Journal (2013). Vitamin D Deficiency and Chronic Neck/Back Pain. (Vitamin D deficiency can cause or worsen chronic musculoskeletal pain and muscle spasm; correcting deficiency often improves neck/back pain)thepermanentejournal.org
Harvard Health (2019). Vitamin B12 Deficiency Can Be Sneaky. (B12 deficiency symptoms include numbness or tingling in hands/feet; neurological deficits from low B12 can manifest as unusual neck pain or extremity tingling)health.harvard.edu
Harvard Health (2020). Can Diet Heal Chronic Pain? (Chronic pain is linked to persistent inflammation; a pro-inflammatory diet (high in sugar, refined carbs, bad fats) can worsen pain, while an anti-inflammatory diet can help reduce it)health.harvard.edu
Harvard Health (2017). Strength Training Relieves Chronic Neck Pain. (Mounting evidence shows targeted exercises to strengthen neck and upper back muscles can break cycles of chronic neck pain and improve posture)health.harvard.edu
Verywell Mind – Wisner, W. (2025). Stress Relief with Meditation. (Mindfulness meditation over 6 weeks significantly decreased perceived stress and improved participants’ ability to manage tension-related symptoms)verywellmind.com
Pharmacally (2023). Chamomile Extract for Anxiety & Sleep. (Chamomile contains apigenin which binds to benzodiazepine receptors, providing calming, mild sedative and muscle-relaxant effects to improve sleep quality and reduce anxiety)pharmacally.com
Caudal, D. et al. (2018). Valerian Extract as a Muscle Relaxant – J. Trad. Complem. Med. (Research confirmed Valerian officinalis root extract had a clear skeletal muscle relaxant effect in mice, suggesting potential to support muscle relaxation in humans)pmc.ncbi.nlm.nih.govpmc.ncbi.nlm.nih.gov
Prime Scholars (2021). Lavender Oil & Muscle Tension. (Study found combining deep breathing relaxation with lavender aromatherapy helped reduce muscle tension and anxiety, providing calm and loosening tight muscles)primescholars.com
McFarlin, B.K. et al. (2016). Turmeric (Curcumin) and Exercise Recovery – J. Diet. Suppl. (Turmeric/curcumin supplementation in athletes reduced post-exercise muscle soreness and inflammatory marker CRP, indicating anti-inflammatory support for muscles)pmc.ncbi.nlm.nih.gov
Camerlin, A. (2020). Arnica for Muscle Pain – Front. Pharmacol. (Review shows topical arnica has anti-inflammatory and analgesic properties; trials found arnica gel significantly reduced pain and swelling in muscle injury and osteoarthritis)sciencedirect.com
Cleveland Clinic (2023). Signs of Meningitis – Muscle Stiffness. (Neck stiffness with fever and headache is a red flag for meningitis and needs immediate medical attention)my.clevelandclinic.org
Nura Pain Clinics (2022). Psychological Impact of Chronic Pain. (Chronic pain often leads to strained relationships, social withdrawal, and emotional distress; recognizing this can encourage seeking support and communicating needs)nuraclinics.com
Bushnell, M.C. et al. (2013). Cognitive and Emotional Control of Pain – Neuron. (Chronic pain negatively affects emotional well-being and cognitive function (attention, memory)pmc.ncbi.nlm.nih.gov; mood disorders can also exacerbate pain – underscores importance of pain management for mental health)pmc.ncbi.nlm.nih.gov