

Between Saturdays: What Your Body Already Knows
From the gym supplement quietly building your brain, to why half of young adults are lonely in a world more “connected” than ever. Four things the research covered this week that are worth your time.

There’s a running theme in this edition: things that are happening in your body that nobody thought to tell you. The supplement that’s been sold as a gym tool for thirty years and is only now being seriously studied as a mental health intervention. The way your menstrual cycle affects your joint vulnerability in ways that sports medicine has ignored for decades. The loneliness data that challenges every assumption about what digital connection actually does for health. And a finding that reframes what your gut microbiome is actually doing for your mood.
Let’s get into it.
Caught My Eye…
Creatine Isn’t Just for the Gym. The Brain Research Is Starting to Land.
If creatine is in your awareness at all, it’s probably as a bodybuilding supplement aka the thing that makes muscles bigger, associated with guys at the gym. The marketing has been so effective at positioning it that most women don’t consider it, and most people don’t know what it actually does.
Here’s what it actually does: creatine is a naturally occurring compound that serves as an energy buffer in cells with high energy demands. In muscle cells, it replenishes ATP (the currency of cellular energy) during high-intensity bursts of effort. In brain cells, it does the same thing, and the brain has extremely high energy demands.
The research on creatine and mental health has been accumulating for several years. What arrived this month is a more complete picture.
A systematic review published in the Canadian Journal of Psychiatry in January 2026, covering five RCTs totalling 238 participants, found that creatine monohydrate as an adjunct treatment for major depressive disorder outperformed placebo in several trials. In the most compelling single study; a 2012 trial by Lyoo et al. testing creatine as an add-on to SSRI treatment in 52 women with major depressive disorder, creatine produced significantly greater improvements in depression scores compared to SSRI plus placebo, with effects visible by week two. The effect size was Cohen’s d = 1.13 at eight weeks, which in psychiatric research terms is substantial.
A 2025 trial published in European Neuropsychopharmacology found that adding creatine to cognitive behavioural therapy significantly improved depression scores compared to CBT plus placebo. And neuroimaging research has found that depression is associated with lower brain phosphocreatine levels, meaning creatine supplementation may be working by restoring something that’s genuinely depleted.
There’s also an important reason this is specifically relevant for women. A 2025 review in Frontiers in Nutrition noted that women naturally produce less creatine than men, and that hormonal changes across the menstrual cycle and through perimenopause further reduce creatine synthesis. Women in the late luteal phase — when mood is typically lower may have a particularly elevated creatine deficit relative to their needs.
What the evidence is not saying: creatine is not an antidepressant, and a November 2025 meta-analysis in the British Journal of Nutrition found the overall effect on depressive symptoms to be below the clinical relevance threshold across studies meaning the average effect is real but modest. It’s not replacing therapy or medication. It’s an adjunct with a plausible mechanism and an accumulating evidence base, in a population (women) that has been almost entirely absent from the research until very recently.
The dose in clinical trials: 3–5g of creatine monohydrate per day. Same form sold in any sports supplement store. Extremely safe. No evidence of harm at standard doses across decades of research.
The practical note: if you’re a woman who trains, takes your mental health seriously, or just wants to hedge against the brain energy deficit that appears to track with low mood and hormonal fluctuation, the case for creatine is no longer just about muscle.
Your Menstrual Cycle Affects Your ACL Risk. Sports Medicine Has Known This for Years and Done Almost Nothing About It.
This one frustrated me the more I read it.
Female athletes tear their ACL at two to eight times the rate of male athletes in equivalent sports. This disparity has been documented since the 1970s. For most of that time, it was attributed to anatomical differences, women’s hips, women’s knees, the Q angle. Biomechanics. Structure.
The hormonal dimension has been understood for years and is only now beginning to enter sports medicine in any meaningful way.
The mechanism: estrogen peaks in the late follicular phase, around ovulation, and this rise increases the expression of relaxin receptors throughout the body. Relaxin is a peptide hormone that activates enzymes called matrix metalloproteinases (MMPs), the same enzymes that break down collagen. In ligament tissue, this means that at the point in the cycle when estrogen and relaxin are highest, collagen synthesis in the ACL is suppressed and collagen degradation is accelerated. The ligament becomes measurably more lax. Joint stability is reduced.
A systematic review published in Healthcare in May 2025 examined injury risk and well-being across the menstrual cycle in young elite female athletes, finding that injury patterns did track with cycle phase. Multiple earlier studies found higher ACL injury incidence around ovulation, when estrogen and relaxin are at their peak.
The important caveat: the research is not conclusive. There are conflicting studies with some finding higher injury risk at ovulation, others in the early follicular phase, others in the late luteal phase. The methodology across studies is inconsistent; most relied on self-reported cycle phase rather than hormonal confirmation. A 2025 commentary in Sports Health called for much better study design to actually resolve the question.
What is clear: the ACL contains hormone receptors. Male ACLs largely don’t. The ligament is hormonally responsive tissue and it changes across the cycle. The research on exactly when risk peaks is not settled — but the fact that risk varies with cycle phase is better established than most athletes or coaches know.
What this means practically is modest but real: if you play sports with high change-of-direction demands like football, basketball, tennis, climbing, skiing being aware that your joint laxity and neuromuscular control fluctuate across the month is useful information. More deliberate warm-up during high-risk phases. Neuromuscular training (specific landing and cutting technique drills) has the best evidence base for ACL prevention in female athletes and is effective regardless of cycle phase. And if you’ve had ACL issues before, this is a conversation worth having with a physio who’s familiar with the hormonal dimension.
What it also means is that the 2-to-8-fold higher ACL injury rate in women has probably been undertreated with structural interventions, better boot design, better landing mechanics while a hormonal dimension that’s been documented for decades has received almost no clinical attention.
Half of Young Adults Are Lonely. And the Research on Why Social Connection Matters Has Reached a Different Level.
In June 2025, the WHO Commission on Social Connection released its global report. The headline: 1 in 6 people worldwide is currently affected by loneliness. New estimates suggest loneliness contributes to approximately 871,000 deaths annually, around 100 deaths every hour.
The statistics on young people were the ones that stopped me. Between 2014 and 2023, the highest rates of loneliness were in adolescents (20.9% of 13-17 year olds) and young adults (17.4% of 18-29 year olds), not older adults, despite the widespread assumption that elderly people are most at risk. The more technologically connected a generation is, the lonelier it appears to be.

A March 2026 study from Washington University in St. Louis surveying 3,000+ young adults across eight countries found that nearly half reported loneliness, and confirmed the cross-national nature of the association with depression and anxiety. This isn’t a US problem or a post-pandemic anomaly. It’s a pattern in the demographic that spends the most time online.
The health evidence on what loneliness does to the body is now at a level where it should probably reshape how we think about public health. Meta-analyses have found that social isolation increases mortality risk by 29%, loneliness by 26%, and living alone by 32%, effects of a similar magnitude to smoking 15 cigarettes per day, as the US Surgeon General’s Advisory noted. Loneliness elevates inflammatory markers, disrupts cortisol rhythm, impairs sleep quality, and increases the risk of cardiovascular disease and type 2 diabetes through multiple pathways.
The mechanism relevant for this audience: loneliness activates the HPA axis. It is a chronic low-level stressor on the stress response system — elevating cortisol, maintaining hyperarousal, fragmenting sleep. The body treats social isolation as a threat to survival (which, evolutionarily, it was). The consequences; anxiety, low mood, poor sleep, increased inflammation, these are not psychological reactions to feeling lonely. They’re physiological responses to a detected threat.
A 2025 Cigna survey of 7,500 US adults found 57% reported loneliness. Younger generations were lonelier than older ones. Gen Z workers reporting loneliness at 72%. Online connection is not substituting for in-person connection in any way that registers in the body’s social signalling systems.
This isn’t a lecture about phones. It’s a data point: in-person social connection is a physiological need with measurable health consequences when unmet. The research has moved past the point where it can be treated as a soft outcome.
Your Gut Microbiome and Your Hormones Are Having a Conversation. The Mental Health Implications Are Significant.
This is the emerging story that hasn’t broken into mainstream wellness content properly yet, and it should have.
A systematic review and meta-analysis published in Healthcare in November 2025 examined the evidence from 28 randomised controlled trials on gut microbiome-targeted interventions like probiotics, prebiotics, synbiotics and their effects on mental health symptoms in women during key hormonal transitions: the premenstrual period, pregnancy, and menopause.
The findings were clinically relevant. Across multiple trials, gut microbiome interventions significantly improved depression and anxiety symptoms in premenstrual women, pregnant women, and women going through menopause. The effect was consistent enough across studies that the authors concluded the gut microbiome is “a promising target for advancing women’s mental health.”
Why this makes sense: the gut microbiome produces approximately 90-95% of the body’s serotonin. It produces GABA. It produces short-chain fatty acids that directly influence brain function and inflammation. The gut-brain axis — the bidirectional communication network between the gut and the central nervous system, means that gut composition directly affects neurotransmitter availability and inflammatory signalling in the brain.
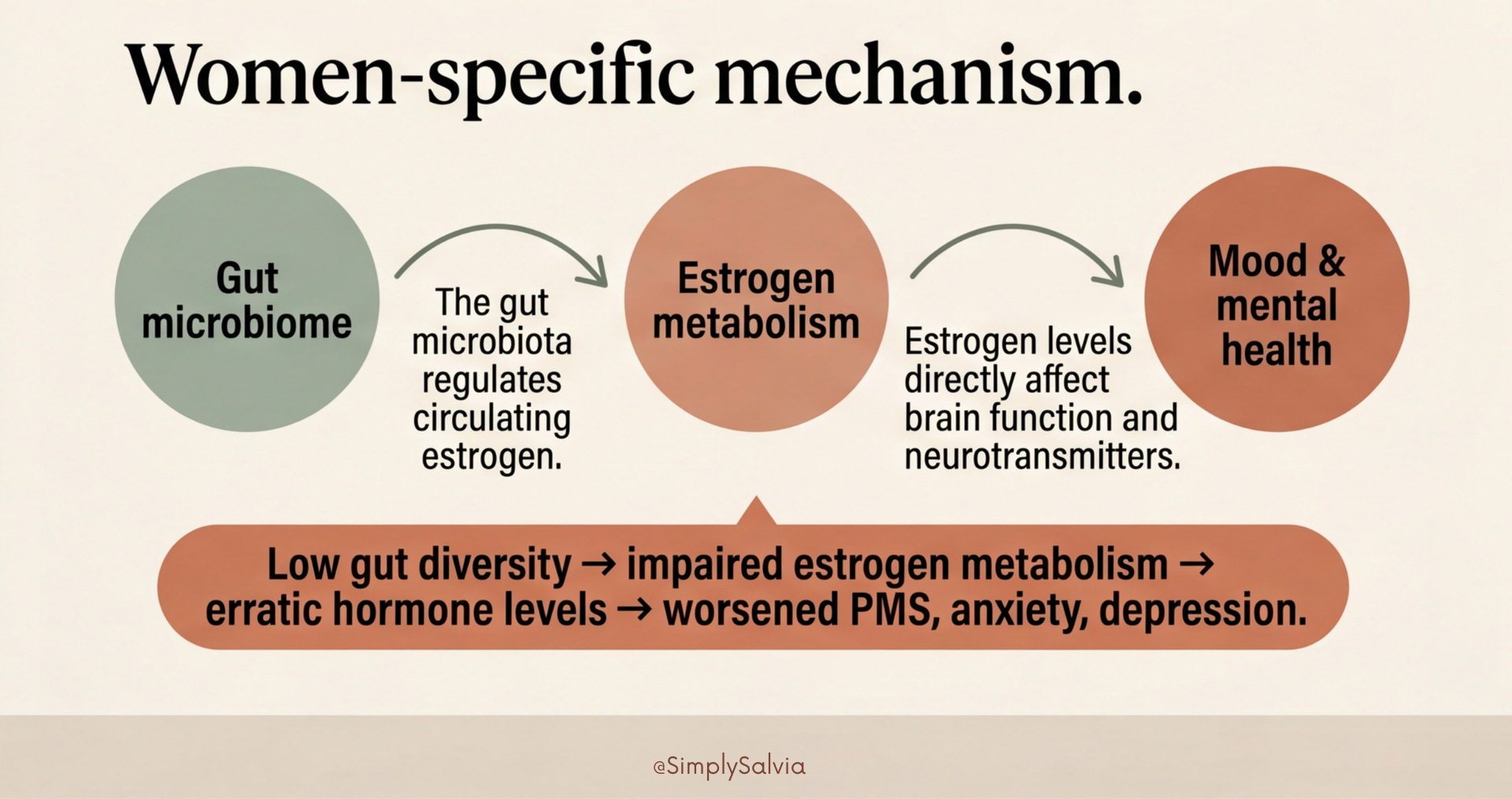
What makes this specifically a women’s health story rather than a general one: female hormones and the gut microbiome have a two-way relationship. Estrogen is metabolised partly in the gut by a set of bacteria collectively called the “estrobolome.” When gut diversity is low, estrogen metabolism is impaired, and circulating estrogen levels become more erratic. This worsens premenstrual symptoms, disrupts the hormonal balance of the cycle, and the research is now suggesting that it directly affects mood and anxiety through gut-brain pathways.
The practical takeaway is not a specific probiotic brand. The dietary pattern that most consistently supports a diverse and healthy gut microbiome — high fibre from varied plants, fermented foods, reduced ultra-processed food is associated with better hormonal regulation and lower rates of depression and anxiety in women. The effect isn’t dramatic and it isn’t immediate. It’s a background intervention that takes weeks to months to manifest. But it’s one of the few dietary changes with a plausible mechanism connecting it directly to both hormonal balance and mental health.
The one specific strain with growing evidence for women specifically: Lactobacillus gasseri CP2305, which in a study of women with premenstrual symptoms improved mood, reduced stress and anxiety, improved sleep, and in one study improved skin appearance. This is an area to watch rather than a recommendation. The research is preliminary and probiotic research has a history of not replicating but the direction of the evidence is interesting.
The information in this post is for educational and informational purposes only. None of the above constitutes medical advice. Always consult a qualified healthcare professional for personal health concerns.
Between Saturdays is a weekly research roundup from Simply Salvia. Four things from science and wellness worth knowing about. If someone sent this to you, you can subscribe.
Detailed Readings:
Creatine for Mental Health: What the Research Shows
Creatine in women’s health: bridging the gap from menstruation through pregnancy to menopause
Menstrual Cycle Hormone Relaxin and ACL Injuries in Female Athletes: A Systematic Review
Social connection linked to improved health and reduced risk of early death
Nearly half of young adults report loneliness in eight-country study
Loneliness and social isolation as risk factors for mortality: a meta-analytic review