

Between Saturdays: The Research They Didn’t Want You to See
From the supplement destroying your sleep to the perimenopause symptoms already showing up in women in their 30s — four things the wellness algorithm isn’t telling you this week.

This edition is a little heavier than usual. Not because the news is all bad, some of it is genuinely useful but because two of this week’s topics are things the healthcare system is actively failing to communicate to women our age. And the other two are things the wellness industry is getting substantially wrong.
Let’s get into it.
Caught My Eye…
Your Pre-Workout Is Probably Ruining Your Sleep. Here’s the Research.
If you take a pre-workout supplement before evening training or anytime after about 3pm, there’s a good chance it’s affecting your sleep more than you realise.
A study published in Sleep Epidemiology in December 2025 from researchers at the University of Toronto analysed data from 912 participants aged 16 to 30. The finding: people who had used pre-workout supplements in the past year were more than twice as likely to report sleeping five hours or less per night compared to those who hadn’t. That’s not a marginal difference, five hours or less is well below the 7-9 hours recommended for this age group and sits in a range that sleep researchers consistently describe as a clinically significant risk to mental health, immune function, and long-term cardiovascular health.
The mechanism isn’t mysterious. Pre-workout formulas typically contain between 90 and 350mg of caffeine per serving. For reference: a cup of coffee contains roughly 100mg, a can of Coke roughly 35mg. Some of the most popular pre-workouts — Bang!, C4, Jack3d, sit toward the higher end. Caffeine has a half-life of approximately 5-7 hours, which means a 200mg serving taken at 6pm still has 100mg active in your system at midnight.
The researchers were careful not to frame this as “stop exercising,” the point isn’t that the training is the problem. It’s that the supplement being used to fuel it may be quietly dismantling the recovery that makes the training worthwhile in the first place.
If you use pre-workout: take it at least 12-14 hours before you need to sleep, check the caffeine content specifically (it varies dramatically between products), and consider whether a lower-stimulant or stimulant-free version achieves the same outcome for afternoon or evening sessions.

Over Half of Women in Their 30s Are Already Experiencing Perimenopause Symptoms. Most Don’t Know It.
This one sat with me for a while after I read it.
A study published in npj Women’s Health in February 2025, led by researchers at UVA Health and the University of Virginia, surveyed more than 4,400 American women aged 30 and older about perimenopausal symptoms. What they found challenged the assumption that perimenopause is something that happens in your late 40s or 50s.
Among women aged 30-35, 55.4% reported symptoms that met the criteria for “moderate” or “severe” on the Menopause Rating Scale, a validated clinical tool used to measure perimenopause symptom burden. That figure rose to 64.3% in women aged 36-40.
Here’s the part that matters most for a younger audience: the symptoms that arrive first are not the ones we associate with menopause. Hot flashes and night sweats, the classic markers most women expect peak at ages 51-55 and were lowest in the 30-35 group. What appears early, years or even decades before those physical symptoms, are psychological symptoms: anxiety, irritability, and depression. These peaked in women aged 41-45 in the study but were already measurable in women in their 30s.
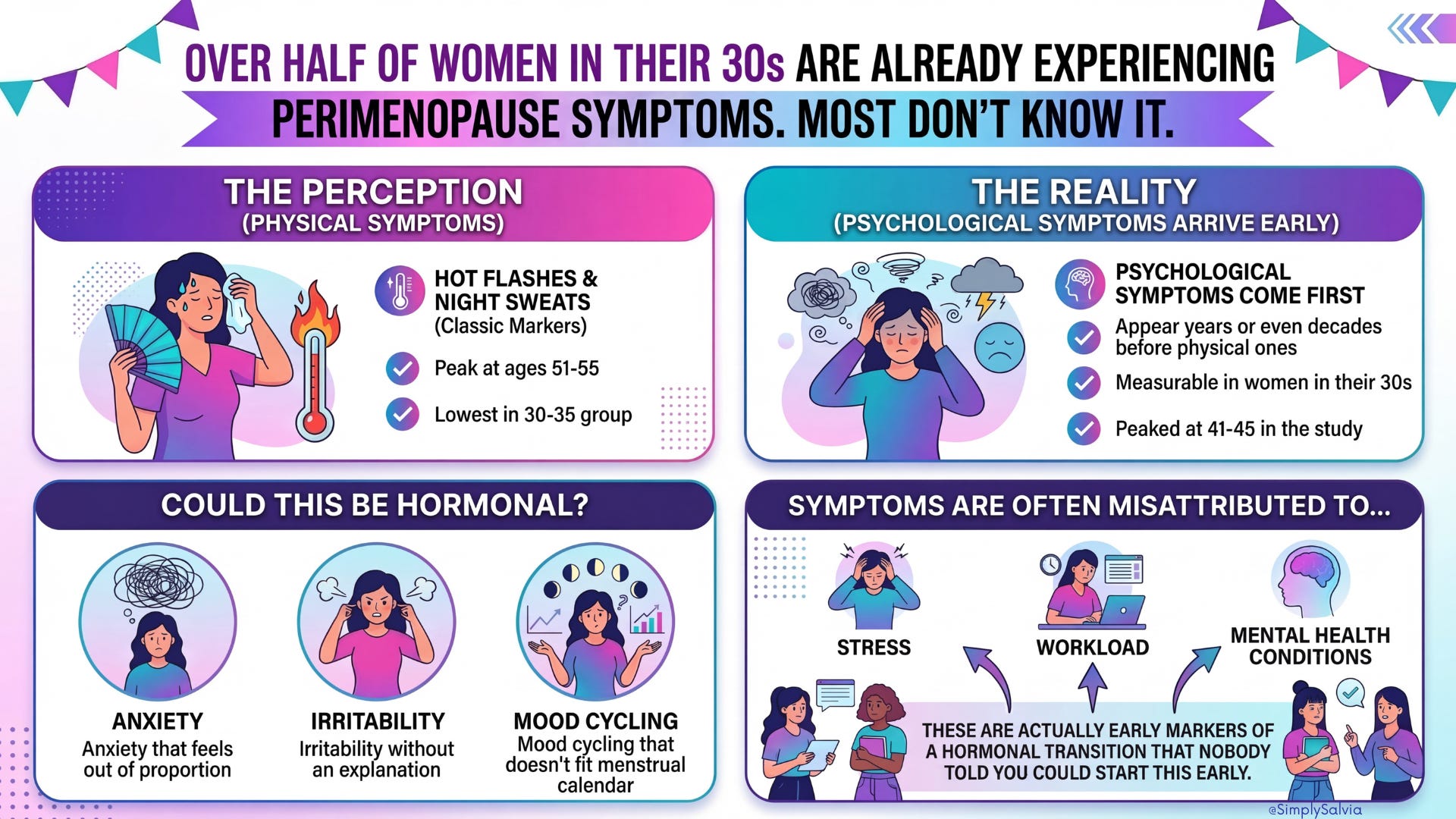
Which means: the anxiety that feels out of proportion. The irritability that doesn’t quite have an explanation. The mood cycling that doesn’t map neatly onto your menstrual calendar. For some women, these are being attributed to stress, workload, or mental health conditions. When they are actually early markers of a hormonal transition that nobody told them could start this early.
The researchers called the gap in awareness and medical education “alarming.” Over 90% of women in the study who experienced symptoms eventually sought medical care but the median age at which women first see a doctor about these symptoms is 56. Decades after the symptoms can start.
If you’re in your 30s and experiencing unexplained mood instability, irregular cycles, changes in sleep, or brain fog that doesn’t track with your obvious life stressors — it is worth raising hormones specifically with your GP. Ask about oestrogen and progesterone levels, and ask whether perimenopause should be on the differential.
If you are suspecting perimenopause maybe this can help:
Short Dive: Is This Perimenopause?

Perimenopause is the natural transitional phase before menopause when a woman’s body begins the shift toward the end of fertility. Unlike puberty, which has a clear beginning and end, perimenopause can feel like an uncertain, drawn-out journey. Hormone levels start fluctuating, and what used to be a regular monthly cycle often turns unpredictable. Many women in their 40s (sometimes as early as their 30s or as late as their 50s) notice their periods becoming irregular as one of the first signs. This stage isn’t “just in your head” or something to simply endure, it’s a real biological process with very real effects on the mind and body.
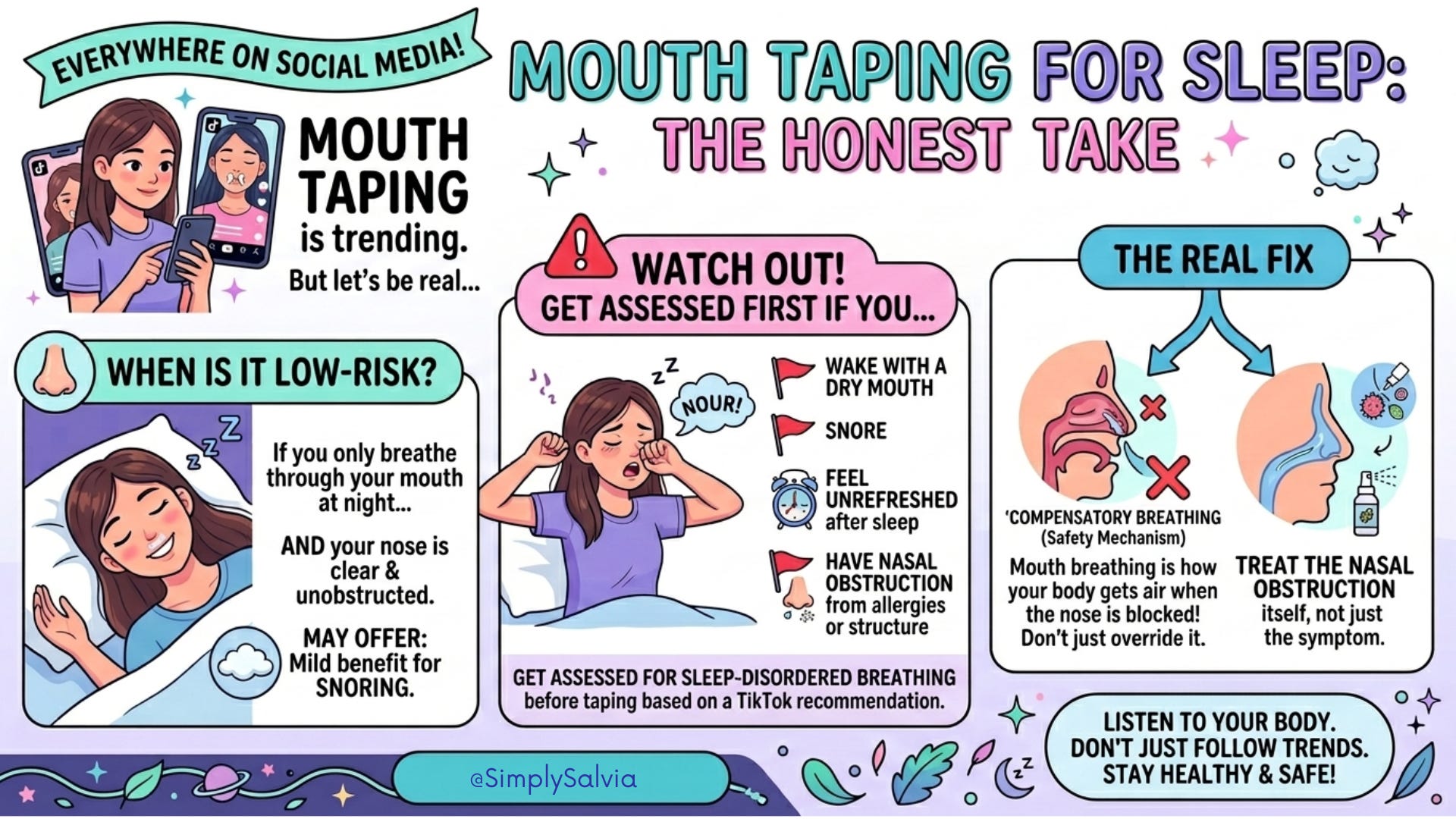
Mouth Taping: What the Systematic Review Actually Found
Mouth taping for sleep is everywhere. The premise: tape your mouth shut at night to force nasal breathing, improving sleep quality, reducing snoring, and fixing a range of respiratory and cognitive issues. This has accumulated tens of millions of views and spawned an entire product category.
The nasal breathing rationale is scientifically sound. Nasal breathing filters, warms, and humidifies air, produces nitric oxide that improves oxygen uptake, and during sleep, upper airway resistance is significantly lower through the nasal route than the oral one, which means nasal breathing is genuinely better for sleep architecture and reduces the risk of airway obstruction.
The question is whether taping your mouth shut is a safe and effective way to achieve that.
A 2025 systematic review published in PLOS One, conducted by researchers at London Health Sciences Centre in Canada, reviewed 10 studies on oral occlusion during sleep. Their conclusions were more cautious than the TikTok content suggests.
For people with mild obstructive sleep apnea who are already primarily nasal breathers, some studies showed minor improvements in apnea-hypopnea index and snoring index. But for people who breathe through their mouth because their nasal passages are obstructed, due to allergies, a deviated septum, enlarged adenoids, chronic congestion, mouth taping doesn’t solve the problem. It removes the compensatory mechanism the body is using to get enough air. The researchers identified potential for serious harm in this group, including asphyxiation risk. The evidence for clinical benefit outside of mild apnea was minimal and not statistically significant.
The honest version: if you breathe through your mouth at night and your nose is clear and unobstructed, mouth taping is probably low-risk and may offer mild benefit for snoring. If you wake with a dry mouth, snore, feel unrefreshed after sleep, or have known nasal obstruction from allergies or structural causes, get assessed for sleep-disordered breathing before taping your mouth shut based on a TikTok recommendation. The correct intervention for nasal obstruction is addressing the obstruction, not overriding the compensatory mouth breathing.
The Largest Women’s Health Study in US History Just Lost Its Funding. Here’s Why It Matters.
This one isn’t a myth-bust or a new discovery. It’s a news item but it’s one that matters specifically for what it means for women’s health research going forward.
The Women’s Health Initiative (WHI) — a landmark longitudinal study that has followed more than 161,000 women since the early 1990s, was informed in April 2025 that the Department of Health and Human Services would terminate its regional centre contracts as part of the broader NIH budget cuts. After significant public and congressional pushback, some of those contracts were reportedly reversed but the situation remains uncertain, and the study’s coordinating centre has been operating without confirmed funding clarity.
Why does this matter for women aged 15 to 35?
The WHI has been the single most influential source of evidence on women’s cardiovascular health, bone density, cancer risk, and hormone therapy safety. It’s the study that transformed HRT prescribing globally, preventing an estimated 126,000 breast cancer cases and 76,000 cardiovascular disease cases over a decade. The participants are now 78-108 years old, providing data on ageing that doesn’t exist anywhere else.
Defunding the WHI doesn’t affect women who are young now in an immediate, visible way. But it does affect the evidence base that will exist when they’re older. Women’s health research has historically been underfunded, under-represented in clinical trials, and routinely dismissed as a lower priority. The WHI was one of the few studies designed from the outset specifically around women’s health outcomes. Cutting it removes decades of longitudinal data collection that can’t be retroactively replaced.
This is the context behind something Melinda French Gates said at the start of this year: that 2026 needs to be the year we “finally stop tolerating women’s suffering.” The research infrastructure to understand that suffering is currently being dismantled.
Worth knowing about. Worth caring about.
Between Saturdays is a weekly research round-up from Simply Salvia. Four things from science and wellness worth knowing about. If someone sent this to you, you can subscribe here.
The information in this post is for educational and informational purposes only. None of the above constitutes medical advice. Always consult a qualified healthcare professional for personal health concerns.
Detailed Readings
Perimenopause symptoms, severity, and healthcare seeking in women in US
Effect of nasal or oral breathing route on upper airway resistance during sleep
HHS Cuts Funding for NIH-Based Women’s Health Initiative Threatening Decades-Long Study