

Between Saturdays: The Food Conversation Nobody’s Having Honestly
From what ultra-processed food is actually doing to your brain chemistry, to why the number on the scale is the wrong measure. Four findings that reframe some very common conversations.

This edition is about food, but not in the usual way. Not macros and meal plans. The more interesting layer: what certain foods are doing to your brain and mood at a chemical level, what the research says about the way we measure progress, why the timing of what you eat matters more than most diet advice acknowledges, and a finding about protein that’s worth knowing if you’ve ever tried to lose weight and been told to eat less and move more. That’s it.
Caught My Eye…
Ultra-Processed Food and Mental Health: The Evidence Has Reached a Different Level
The research on ultra-processed food and mental health has been building for several years. It has now reached a point where it is difficult to describe the findings as preliminary.
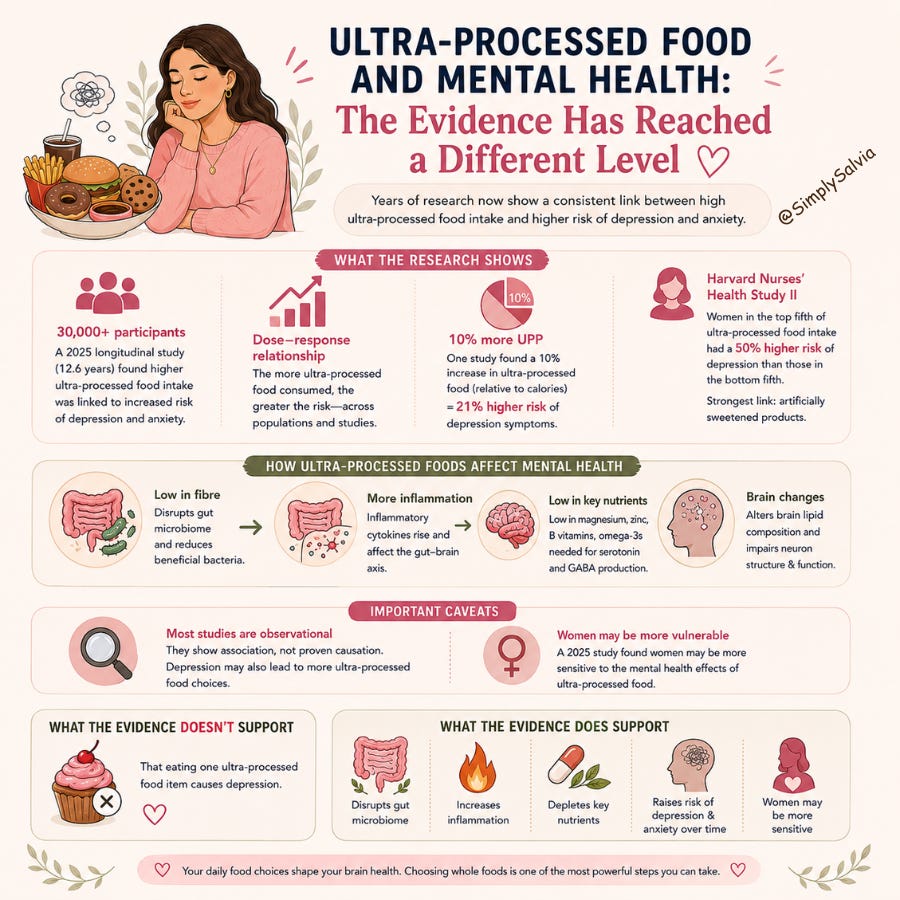
A longitudinal study of over 30,000 participants, published in 2025 and followed over an average of 12.6 years, found that those with high ultra-processed food intake had increased risk of mental disorders including depression and anxiety. A review published in Oxford Journal in August 2025 synthesised multiple large cohort studies and found a consistent dose-response relationship: the more ultra-processed food consumed, the higher the risk of depression and anxiety, across populations and across study designs. One earlier cohort study found that a 10% increase in ultra-processed food intake relative to daily calories was associated with a 21% higher risk of developing depression symptoms over a five-year follow-up period.
The Harvard Nurses’ Health Study II finding is probably the clearest single data point: women in the top fifth of ultra-processed food consumption had a 50% higher risk of developing depression than those in the bottom fifth. The link was particularly strong for artificially sweetened products.
The mechanism runs through several routes simultaneously. Ultra-processed foods are low in the dietary fibre that gut bacteria need to produce short-chain fatty acids, which means the gut microbiome becomes less diverse, inflammatory cytokines rise, and the gut-brain axis produces pro-inflammatory signals in the brain. Ultra-processed foods are also typically low in the micronutrients; magnesium, zinc, B vitamins, omega-3s, that serve as cofactors for neurotransmitter synthesis. Without them, serotonin and GABA production is impaired at the chemistry level.
A scoping review published in Frontiers in Nutrition in January 2026 made the lipid metabolism angle explicit: ultra-processed foods alter brain lipid composition over time in ways that affect the structure and function of neuronal membranes, particularly in regions involved in mood regulation. This is a structural change and not just a nutritional deficiency.
Two caveats worth knowing: most of the studies are observational, meaning they show a consistent association, not a confirmed causal direction. People with depression may also be more likely to reach for ultra-processed food, not only the other way around. A 2025 cross-sectional study in Iran explicitly noted that women may be more vulnerable than men to the mental health effects of ultra-processed food consumption, suggesting the association is sex-specific in ways that warrant further investigation.
What the evidence doesn’t support: the idea that eating one ultra-processed food item causes depression. What it does support: that a diet consistently high in ultra-processed food creates a biological environment, through the gut microbiome, through chronic inflammation, through micronutrient depletion, that makes depression and anxiety more likely over time. And that women, specifically, may be more sensitive to this effect.
The Scale Is the Worst Measure of Progress. Here’s What to Use Instead.

This one is short because it doesn’t need to be long. It needs to be said clearly.
The number on the scale is measuring your total mass — including bone, muscle, organs, water, and the contents of your digestive system at that moment. It is not measuring fat loss. It is not measuring health. It is not measuring body composition. It is not stable from day to day, from morning to evening, or from week one to week two of any given month.
The research on why scales mislead is particularly relevant for women because of water retention. Progesterone promotes fluid retention in the luteal phase, which can add 1–3kg of water weight in the two weeks before a period. This is not fat. It reverses within days of menstruation starting. A woman who has genuinely lost fat and built muscle through three weeks of training can step on a scale in the late luteal phase, see a number higher than when she started, and conclude that nothing is working. When the reality is the exact opposite.
The measures that tell you more:
How your clothes fit: specifically how the waist and hip of the same clothing item sits over time, which is a body composition measure, not a weight measure
Progress photos taken in consistent lighting and positions across weeks and months. Visual changes in body composition that the scale won’t show
Performance measures: how much you lift, how far you walk without fatigue, how your resting heart rate changes over time
Energy and sleep quality: if your energy is higher and your sleep is better, your metabolic health is improving regardless of the scale
How you feel across your cycle: if PMS symptoms are reducing, if energy is more consistent across the month, the dietary and lifestyle changes are working
If you track weight at all, the most useful approach is to weigh in the same conditions daily (same time of day, same level of hydration) and look at the rolling 7-day average rather than the daily number. The 7-day average smooths out the hormonal water retention, the digestive fluctuations, and the noise of day-to-day variation. The trend over 4–8 weeks is the signal. The daily number is mostly noise.
The deeper point: the scale measures one thing (mass) and we use it to measure a completely different thing (progress). These are not the same measure. Replacing a bad measure with better ones is not giving up. It’s doing it properly.
Meal Timing: The Research That Doesn’t Get Enough Attention
The nutritional research has for years focused almost entirely on what to eat. More recently, it’s started asking when, and the findings are interesting enough to be worth knowing.
The short version: when you eat matters, and it matters more in certain windows of the day than others. Here’s the research that’s accumulated:
Breakfast protein reduces post-meal glucose spikes all day.
Studies show that a high-protein breakfast (25g+ of protein) reduces the glucose response not just to that meal but to subsequent meals throughout the day. The mechanism: early morning protein intake primes the insulin response and sets a metabolic tone that carries through. A high-carbohydrate breakfast (cereal, toast, fruit juice) does the opposite. It starts the blood sugar rollercoaster early and the instability compounds.
Insulin sensitivity is highest in the morning, lowest in the evening.
This is a circadian rhythm finding with direct dietary implications. Your body handles carbohydrates more efficiently in the first half of the day than the second. A large, carbohydrate-heavy meal at 9pm produces a larger and more prolonged glucose response than the same meal eaten at 12pm. This is why shifting calorie-dense, carbohydrate-rich eating earlier in the day and making dinner lighter on carbohydrates and heavier on protein and vegetables, supports better metabolic health and body composition without necessarily reducing total calories.
Eating too fast removes the satiety signal.
Satiety hormones (GLP-1, PYY) take approximately 15–20 minutes to reach the brain after eating begins. A meal eaten in 7–10 minutes finishes before the fullness signal arrives. A cohort study of 59,000 people found that self-reported fast eaters had significantly higher rates of metabolic syndrome, independent of total calorie intake. Eating slowly is not a wellness affectation. It’s working with the timing of your own hormones.
Not eating after 8–9pm supports overnight cortisol rhythm and sleep quality.
Late-night eating elevates blood sugar during the overnight period, which can trigger cortisol releases to regulate it (particularly if glucose drops low), which fragments sleep. The same mechanism covered in the Between Saturdays sleep edition: the 3am waking that many women experience in the luteal phase is partly a blood sugar event.
None of this requires a rigid meal schedule. It requires broadly aligning eating with the body’s daily rhythms: protein earlier, carbohydrates earlier, dinner lighter and earlier when possible, and meals eaten slowly enough for the satiety system to do its job.
Why You’re Hungrier in the Second Half of Your Cycle, And Why That’s Not a Flaw
This one is a direct follow-up to the weight loss Short Dive and worth saying again in plain language because it gets misunderstood so consistently.
In the two weeks after ovulation — the luteal phase, your resting metabolic rate increases. Your body is burning approximately 100–500 more calories per day at rest compared to the first half of the cycle. This is driven by progesterone and by the body’s preparation for a potential pregnancy, which requires additional energy reserves. The hunger that goes with this is the body accurately signalling a real increase in energy demand.
Research has confirmed that caloric intake increases by this amount in the luteal phase in studies tracking food intake across the cycle. Women are not imagining the increased appetite. They are not losing their discipline. Their body is asking for more fuel because it is genuinely using more fuel.
The problem is not the hunger. The problem is what tends to satisfy it: high-GI carbohydrates and sugar, because the blood sugar instability of the luteal phase (progesterone promotes mild insulin resistance) drives cravings for fast glucose. Eating more refined carbohydrates in this phase produces bigger blood sugar spikes and crashes, which produce more cravings, which produce more eating. A cycle that has nothing to do with willpower and everything to do with blood sugar chemistry.

The answer is not to resist the hunger. It is to satisfy it with foods that don’t restart the blood sugar loop: protein-dense meals, complex carbohydrates with fibre, fat sources that slow digestion. Eating more in the luteal phase is appropriate. Eating more chocolate and crisps specifically because the blood sugar crash is signalling an emergency is the version that’s worth redirecting.
If you track your intake and see a consistent increase in the luteal phase every month, that’s not failure. That’s the data confirming what the research says. The goal is to meet the increased energy demand in a way that doesn’t compound the blood sugar instability that’s already making this phase harder.
The information in this post is for educational and informational purposes only. None of the above constitutes medical advice. Always consult a qualified healthcare professional for personal health concerns.
Between Saturdays is a weekly research roundup from Simply Salvia. Four things from science and wellness worth knowing about. If someone sent this to you, you can subscribe here.
Detailed Readings
The Impact of Ultra-Processed Foods on Depression and Anxiety: A Literature Review
Ultra-Processed Foods and Mental Health: What the Research Actually Says
Ultra-processed foods may increase risk of depression
Dietary energy intake across the menstrual cycle: a narrative review