

Between Saturdays: Not Just a Bad Period
From research finally calling endometriosis what it actually is, to why your ADHD symptoms might be tracking your cycle in ways nobody's told you. Four findings reshaping how we understand conditions.

This edition has a theme, even though I didn’t plan it that way: conditions in women that have been minimised, misdiagnosed, or treated as “just” something - just a bad period, just being scattered, just stress. When the research increasingly shows something more specific and more systemic underneath. Endometriosis is having its biggest research moment in years. ADHD in women is finally being studied across hormonal transitions instead of just childhood. And two more findings that explain things many of you have lived with but never had a name for.
Caught My Eye…
Endometriosis Isn’t a Reproductive Disease. It’s a Whole-Body Inflammatory Disease. And That Reframe Changes Everything.
For decades, endometriosis has been treated as a gynaecological condition - tissue similar to the uterine lining growing where it shouldn’t, causing pain, mainly during periods. A research finding from March 2026 is pushing the field toward a fundamentally different understanding, and the implications are significant.
A study found that people with endometriosis were about twice as likely to be diagnosed with an autoimmune disease, such as lupus or multiple sclerosis, within two years of their endometriosis diagnosis. This doesn’t mean endometriosis is itself an autoimmune disease but it suggests the two share underlying problems, including ongoing inflammation and changes in immune system function.
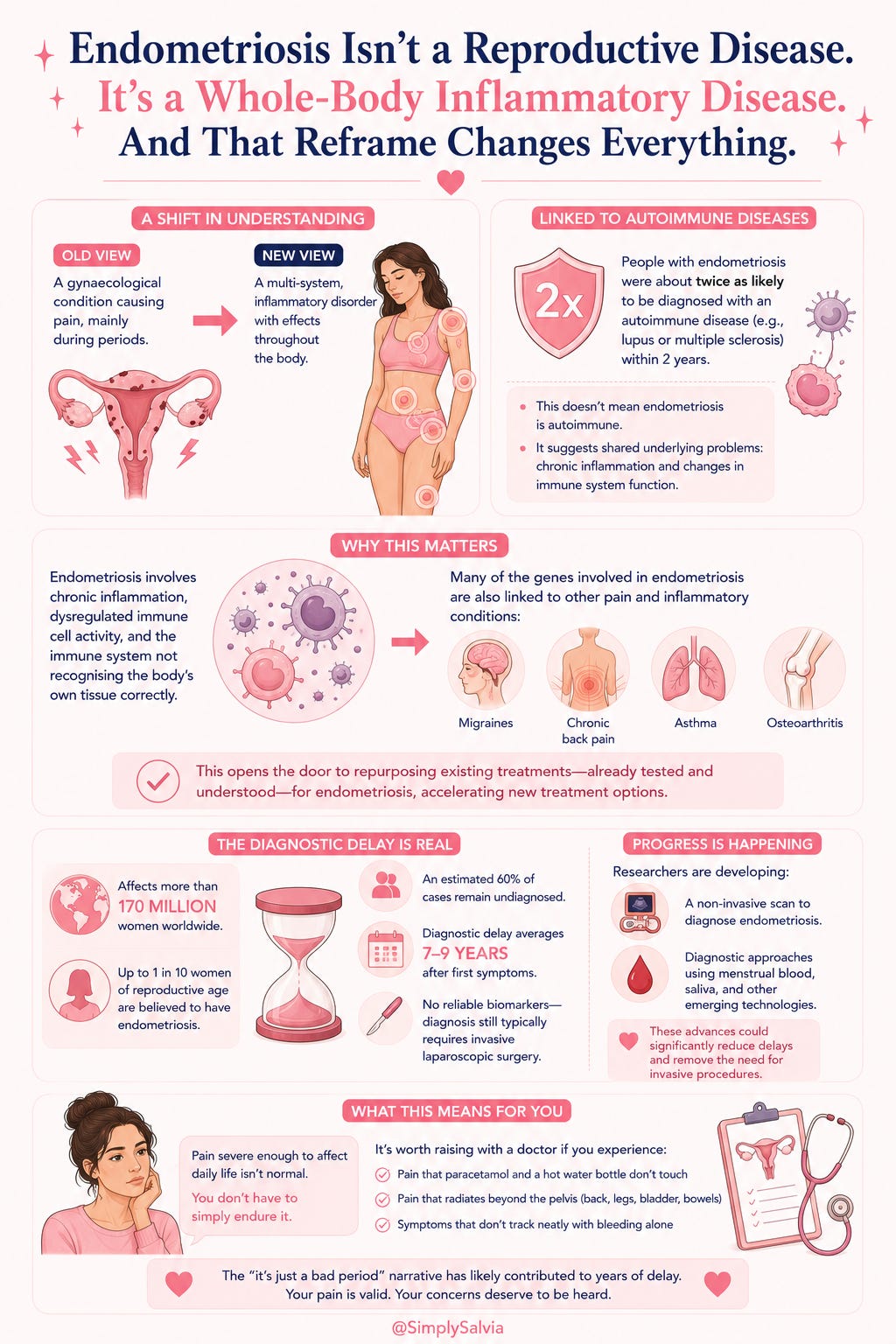
A growing body of research now shows that endometriosis is not solely a reproductive condition or a “bad period.” It’s a multi-system, inflammatory disorder with effects throughout the body. The overlapping features; chronic inflammation, dysregulated immune cell activity, and problems with the immune system recognising the body’s own tissue correctly, strengthen the case for understanding it as a systemic immune disorder.
This matters beyond academic classification. Many of the genes involved in endometriosis are also linked to other pain and inflammatory conditions; migraines, chronic back pain, asthma, and osteoarthritis. This raises the possibility that existing treatments for those conditions, already tested and understood, could be repurposed for endometriosis, a much faster path to new treatment options than starting from scratch.
The diagnostic delay remains one of the most troubling aspects of this condition. Endometriosis affects more than 170 million women worldwide, with up to 1 in 10 women of reproductive age believed to have the condition and yet an estimated 60% of cases remain undiagnosed. Diagnostic delay averages 7 to 9 years after first symptoms, and there are currently no reliable biomarkers meaning diagnosis still typically requires invasive laparoscopic surgery.
There’s real movement on this front too. Researchers are developing a non-invasive scan to diagnose endometriosis, with the potential to significantly reduce diagnostic delays and remove the need for invasive procedures. Globally, research is also exploring diagnostic approaches using menstrual blood, saliva, and other emerging technologies.
What this means if period pain has ever been dismissed as normal: pain severe enough to affect daily function, school, or work is not something you should have to simply endure. The “it’s just a bad period” framing has likely contributed to the diagnostic delay this condition is now infamous for. If your periods involve pain that paracetamol and a hot water bottle don’t touch, pain that radiates beyond the pelvis, or symptoms that don’t track neatly with bleeding alone, this is worth raising directly and specifically with a doctor — not as something to push through.
ADHD Symptoms in Women Change Across the Menstrual Cycle. Almost Nobody Diagnosing ADHD Is Asking About This.
This is one of the more striking research findings to come out this year, and it has real implications for how ADHD is assessed in women.
A world-first study examining ADHD in women across their lifespan found there may be systemic misdiagnosis and underdiagnosis of women rather than ADHD genuinely being more common in men. The standout finding: 88% of women surveyed reported changes in their ADHD symptoms during their menstrual cycle, particularly in the latter two weeks of the cycle aka the luteal phase.
The hormonal mechanism is becoming clearer. Dopamine (one of the neurotransmitters most directly implicated in ADHD) interacts with both estrogen and progesterone. As estrogen rises in the follicular phase, dopamine signalling tends to be more efficient so symptoms often feel more manageable. As estrogen falls in the late luteal phase, that support diminishes, and ADHD symptoms like difficulty concentrating, impulsivity, emotional dysregulation, frequently intensify. This is a distinct and separate phenomenon from generic premenstrual mood changes; it’s a hormonally-mediated fluctuation in symptom severity for a condition that’s already present year-round.
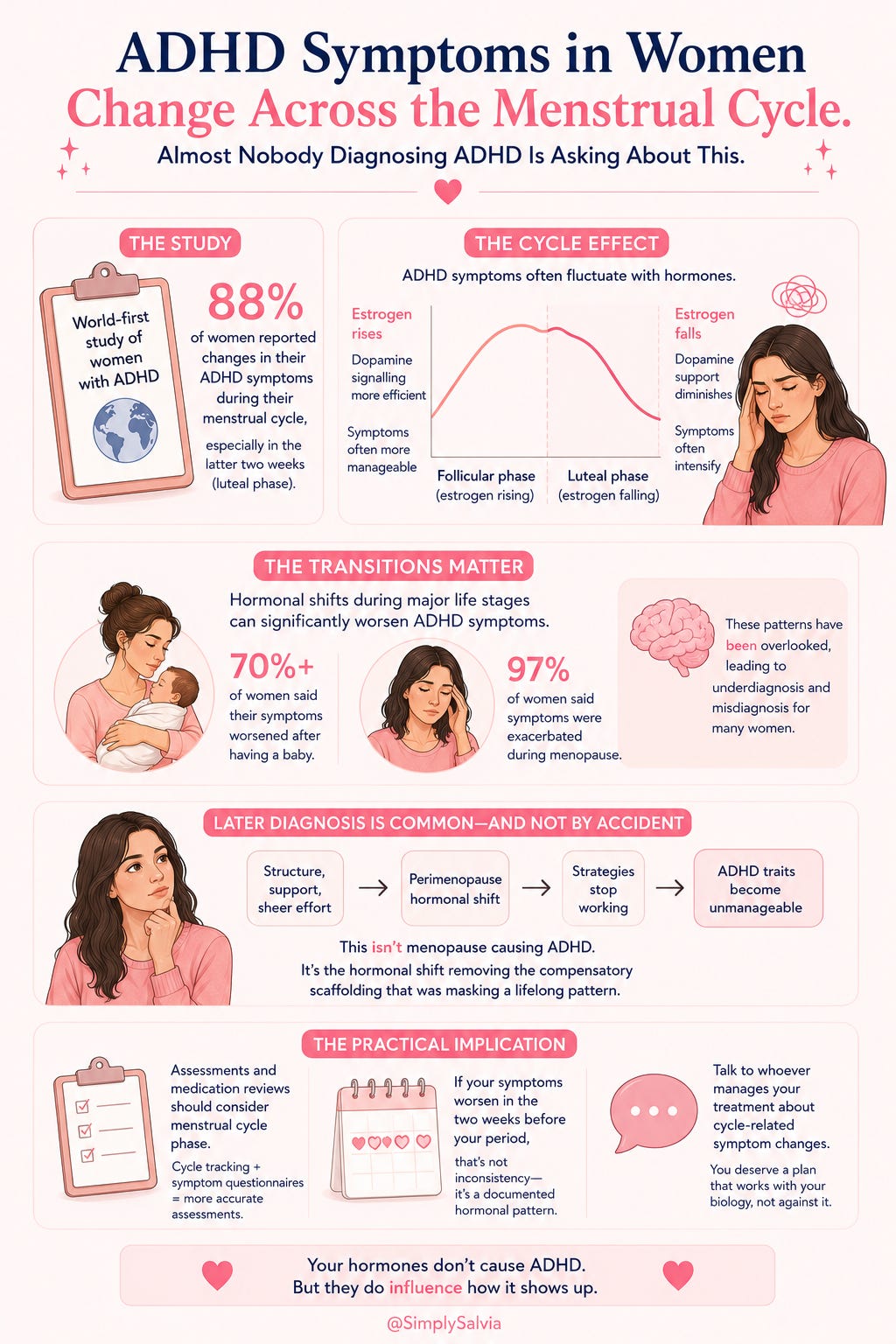
The transitions matter just as much as the monthly cycle. More than 70% of women surveyed said their ADHD symptoms worsened after having a baby, and almost all women (97%) said their symptoms were exacerbated during menopause. ADHD symptoms can worsen during the postpartum period and through perimenopause, accompanied by increased mood and sleep disturbances and these patterns have historically been overlooked, contributing to underdiagnosis and misdiagnosis.
This has a particularly important implication for women diagnosed with ADHD later in life, often in their 30s, 40s, or during perimenopause. Perimenopause can unmask ADHD traits that were previously kept in check by structure, support, or sheer effort. For many women, hormonal change is the first time the strategies that worked for years stop being enough. This isn’t menopause causing ADHD, it’s the hormonal shift removing the compensatory scaffolding that was masking a lifelong pattern.
The practical implication: if ADHD assessment or medication review doesn’t take menstrual cycle phase into account, it may be missing a significant part of the picture. Researchers are now recommending cycle tracking alongside validated symptom questionnaires as part of a more accurate assessment protocol for women. If you’re already diagnosed and notice your symptoms are markedly worse in the two weeks before your period, this isn’t inconsistency in your condition, it’s a documented hormonal pattern worth discussing with whoever manages your treatment.
Heart Disease Risk in Type 2 Diabetes Looks Completely Different in Women Than in Men
This finding deserves more attention than it’s getting. Type 2 diabetes substantially raises cardiovascular risk in everyone but the way that risk plays out, and the symptoms that signal it, differ meaningfully by sex.
A major study covered by ScienceDaily in early 2026 examined how cardiovascular risk in type 2 diabetes diverges between men and women and the differences are significant enough to affect how risk should be screened for and discussed with women specifically. Women with type 2 diabetes have historically been found to lose more of the natural cardiovascular protection that estrogen provides pre-menopause compared to men’s baseline risk trajectory, meaning a diabetes diagnosis can represent a proportionally larger jump in cardiovascular risk for women than the same diagnosis represents for men.
This connects to a pattern that’s been documented across cardiovascular research generally: women’s heart attack symptoms are less likely to be the “crushing chest pain” most people associate with cardiac events, and more likely to present as fatigue, nausea, jaw pain, or breathlessness, symptoms that get attributed to anxiety or stress far more often in women than in men, as covered in an earlier Between Saturdays.
For women with type 2 diabetes, PCOS, or a family history of early cardiovascular disease, this combination, atypical symptom presentation plus a disproportionate cardiovascular risk increase from diabetes is a real gap in standard care. The practical takeaway: a cardiovascular risk conversation with a GP shouldn’t wait for traditional risk factors alone (high cholesterol, smoking, obvious chest symptoms). Family history, PCOS, gestational diabetes history, and blood sugar patterns are all relevant data points worth bringing into that conversation explicitly, particularly for women under 50 who don’t fit the traditional cardiac risk profile.
Menopause and Brain Structure: The Follow-Up Research Is Getting More Specific
I covered the initial February 2026 finding on menopause and grey matter loss in an earlier edition. The research has continued to develop since, and it’s worth a fuller look now that more data exists.
The original study found that menopause is linked to measurable changes in brain structure, with grey matter loss in regions tied to memory and emotional regulation alongside changes in mental health and sleep. Subsequent research from Cambridge has continued to build out this picture, linking the menopausal transition specifically to changes in brain structure, sleep disruption, anxiety, and cognitive symptoms as an interconnected cluster rather than separate, unrelated complaints.
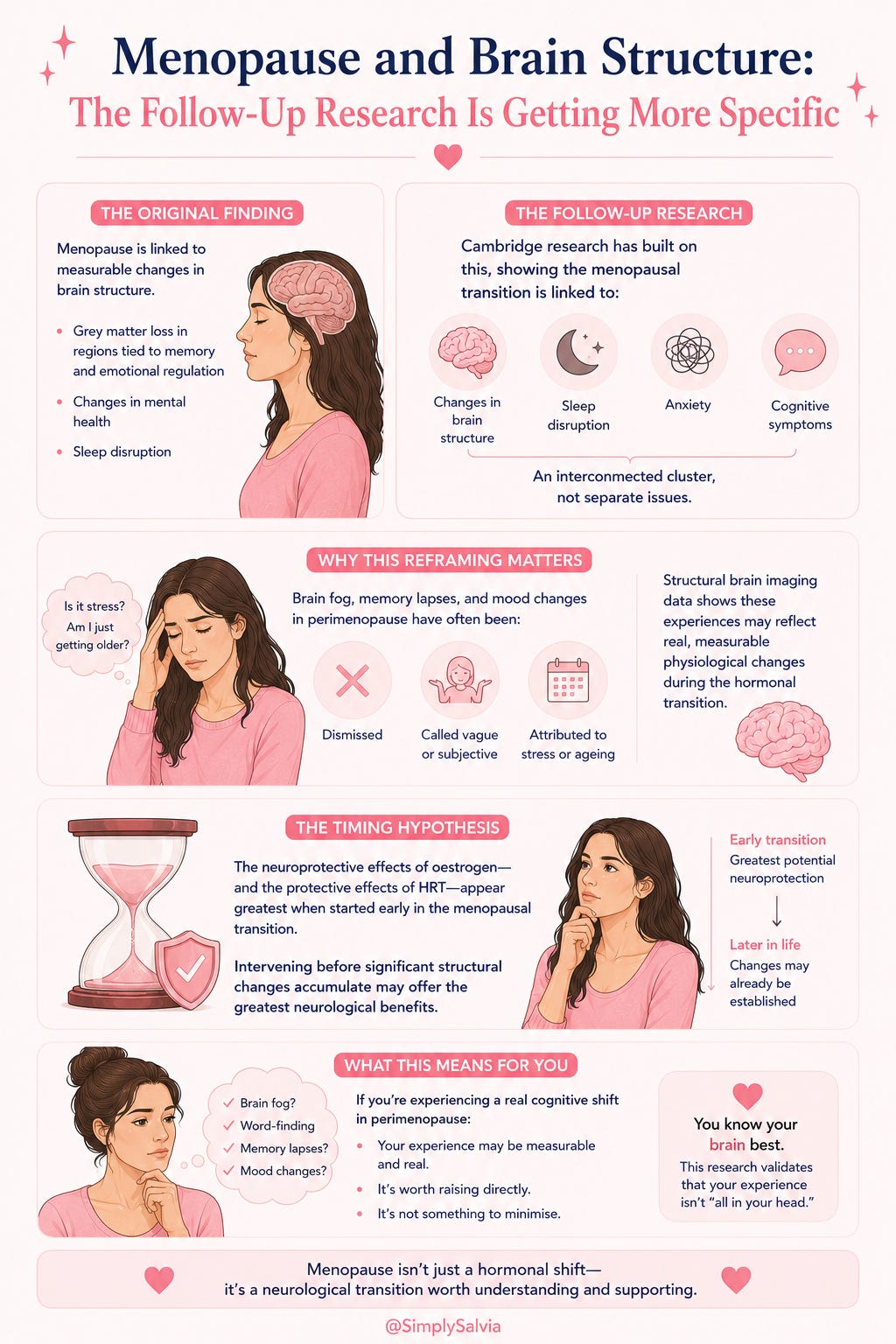
This reframing matters for a specific reason: brain fog, memory lapses, and mood changes during perimenopause have historically been treated as vague, subjective complaints and sometimes dismissed entirely, sometimes attributed to stress or ageing generically. The structural brain imaging data suggests these experiences may reflect real, measurable physiological changes happening during the hormonal transition, not just a subjective shift in how women are coping with midlife generally.
The “timing hypothesis” continues to be the most actionable finding from this research line: the neuroprotective effects of oestrogen and by extension, the protective effects of hormone therapy when started early in the menopausal transition, appear to be greatest when intervention happens before significant structural changes have accumulated, rather than waiting until much later in life. This adds further weight to a conversation we’ve covered before: HRT decisions framed only as a late-life option may be missing a window where the neurological benefits are most significant.
For women in perimenopause experiencing what feels like a real cognitive shift and not “I’m just getting older” but a genuine change in mental clarity, word-finding, or memory this research is validating that the experience may be measurable and real, and is worth raising directly rather than minimising.
The information in this post is for educational and informational purposes only. None of the above constitutes medical advice. Always consult a qualified healthcare professional for personal health concerns.
Between Saturdays is a weekly research roundup from Simply Salvia. Four things from science and wellness worth knowing about. If someone sent this to you, you can subscribe here.
Detailed Readings
Endometriosis: new insights and opportunities for relief of symptoms
ADHD and Sex Hormones in Females: A Systematic Review
Why heart disease risk in type 2 diabetes looks different for men and women